Anna Laws, Michael Allen, Jason Scott, Lisa Moseley, Kerry Pearn, Gary A Ford, Chris Price, Phil White, Graham McClelland, Lisa Shaw, Daniel Phillips, Dave Wilson, Peter McMeekin, Martin James
{"title":"Modelling the potential clinical benefit of mobile stroke units in England.","authors":"Anna Laws, Michael Allen, Jason Scott, Lisa Moseley, Kerry Pearn, Gary A Ford, Chris Price, Phil White, Graham McClelland, Lisa Shaw, Daniel Phillips, Dave Wilson, Peter McMeekin, Martin James","doi":"10.1186/s12873-025-01242-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) are well-established emergency reperfusion treatments for stroke caused by clots. Both reduce disability but effectiveness is highly time-dependent, declining in the first few hours after stroke onset. Mobile stroke units (MSUs) have been proposed as a way of improving outcomes after stroke. MSUs enable on-scene brain imaging and delivery of IVT, and can allow for better choice of destination hospital. The primary objective of the study was to model the likely effect of MSUs on clinical outcomes (the ability to live independently, modified Rankin Scale 0-2) across all of England assuming no resource restrictions during deployment.</p><p><strong>Methods: </strong>We used modelling of times to treatment and outcomes. Modelling was performed for Lower Super Output Areas (LSOAs) in England. Admission numbers were based on Hospital Episode Statistics and travel times estimated from data from Open Street Map. Outcomes were predicted based on times to IVT and MT; we report outcomes as utility or the proportion of patients able to live independently at 3-6 months after stroke. We assumed MSUs and stroke units all had the same propensity to use IVT.</p><p><strong>Results: </strong>For every 100 patients suitable for IVT or MT, there will likely be 1-3 more people who can live independently following MSU care. The benefit comes from both earlier IVT and the direct transfer of patients likely to benefit from MT to their closest MT-centre by avoiding inter-hospital transfers that would be used in usual care. If, as is likely, about 1 in 5 stroke patients are suitable candidates for IVT or MT, an MSU would need to attend approximately 250 stroke patients for every one extra independent-living outcome. If about half of the patients to whom an MSU is dispatched are actual strokes (the others being stroke mimics), an MSU would need to attend approximately 500 patients for every one extra independent-living outcome. Some areas, furthest from where MSUs are based, will receive no benefit from MSU care, whereas other areas may have up to 4 additional independent-living outcomes for every 100 patients suitable for IVT or MT. Quick MSU dispatch and fast on-scene treatment are crucial to achieving the benefit of MSUs, otherwise use of MSUs may have no overall benefit, or worse outcomes, than usual care. The above benefits do not include any other possible benefits unrelated to earlier IVT or MT.</p><p><strong>Conclusions: </strong>This study suggests that the overall benefit of MSU care if deployed across all of England is likely to be modest. Selective use of MSUs in specific areas is likely to be more effective than widespread implementation. Rapid dispatch, fast on-scene treatment of patients, and careful selection of which patients to dispatch the MSU to (by location and confidence in that person being a confirmed stroke patient), are all critical for maximising benefits from MSU care. MSUs should not be seen as an alternative to optimising day-to-day emergency stroke systems.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"111"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12219994/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01242-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) are well-established emergency reperfusion treatments for stroke caused by clots. Both reduce disability but effectiveness is highly time-dependent, declining in the first few hours after stroke onset. Mobile stroke units (MSUs) have been proposed as a way of improving outcomes after stroke. MSUs enable on-scene brain imaging and delivery of IVT, and can allow for better choice of destination hospital. The primary objective of the study was to model the likely effect of MSUs on clinical outcomes (the ability to live independently, modified Rankin Scale 0-2) across all of England assuming no resource restrictions during deployment.
Methods: We used modelling of times to treatment and outcomes. Modelling was performed for Lower Super Output Areas (LSOAs) in England. Admission numbers were based on Hospital Episode Statistics and travel times estimated from data from Open Street Map. Outcomes were predicted based on times to IVT and MT; we report outcomes as utility or the proportion of patients able to live independently at 3-6 months after stroke. We assumed MSUs and stroke units all had the same propensity to use IVT.
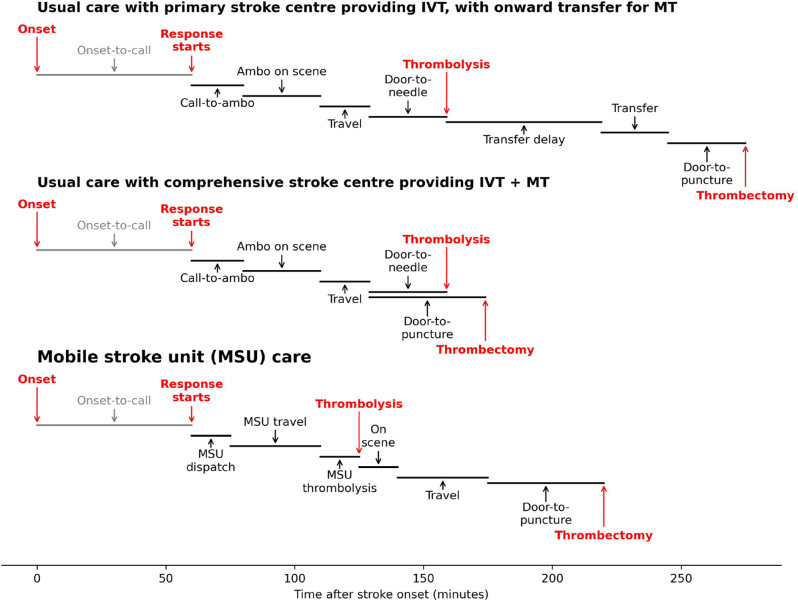
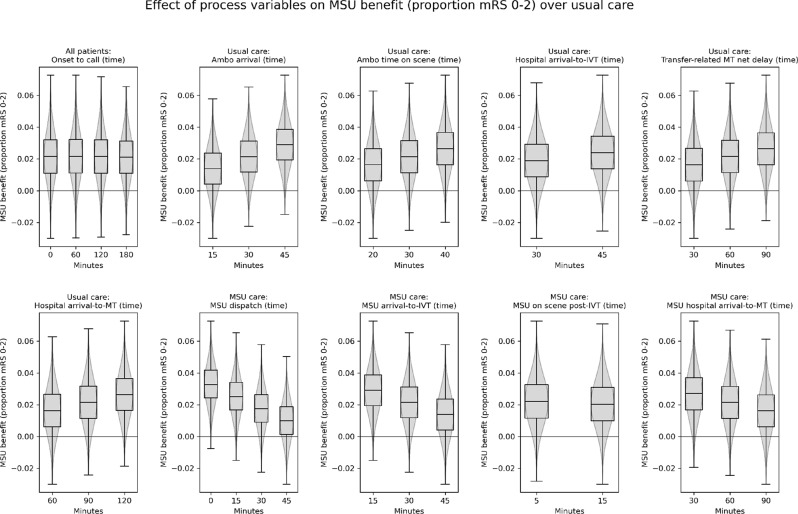
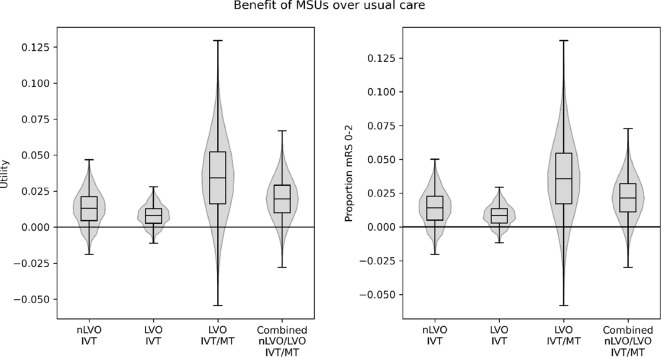
Results: For every 100 patients suitable for IVT or MT, there will likely be 1-3 more people who can live independently following MSU care. The benefit comes from both earlier IVT and the direct transfer of patients likely to benefit from MT to their closest MT-centre by avoiding inter-hospital transfers that would be used in usual care. If, as is likely, about 1 in 5 stroke patients are suitable candidates for IVT or MT, an MSU would need to attend approximately 250 stroke patients for every one extra independent-living outcome. If about half of the patients to whom an MSU is dispatched are actual strokes (the others being stroke mimics), an MSU would need to attend approximately 500 patients for every one extra independent-living outcome. Some areas, furthest from where MSUs are based, will receive no benefit from MSU care, whereas other areas may have up to 4 additional independent-living outcomes for every 100 patients suitable for IVT or MT. Quick MSU dispatch and fast on-scene treatment are crucial to achieving the benefit of MSUs, otherwise use of MSUs may have no overall benefit, or worse outcomes, than usual care. The above benefits do not include any other possible benefits unrelated to earlier IVT or MT.
Conclusions: This study suggests that the overall benefit of MSU care if deployed across all of England is likely to be modest. Selective use of MSUs in specific areas is likely to be more effective than widespread implementation. Rapid dispatch, fast on-scene treatment of patients, and careful selection of which patients to dispatch the MSU to (by location and confidence in that person being a confirmed stroke patient), are all critical for maximising benefits from MSU care. MSUs should not be seen as an alternative to optimising day-to-day emergency stroke systems.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


