Neslihan Ergün Süzer, Gülbin Aydoğdu Umaç, Süleyman Alpar, Sarper Yılmaz
{"title":"Comparison of return of spontaneous circulation prediction scores in patients with cardiac arrest during ambulance transport.","authors":"Neslihan Ergün Süzer, Gülbin Aydoğdu Umaç, Süleyman Alpar, Sarper Yılmaz","doi":"10.1186/s12873-025-01265-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac arrest during ambulance transport is a complex situation that has features of both in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) but lacks a clear classification. This study aimed to evaluate the diagnostic performance of prehospital and in-hospital ROSC prediction tools in patients experiencing cardiac arrest during ambulance transport.</p><p><strong>Methods: </strong>A retrospective study was conducted with patients experiencing cardiac arrest during transport. Demographic, clinical, and treatment data were collected, including pre-arrest consciousness, arrest rhythm, and cardiopulmonary resuscitation duration. Four ROSC prediction scores (Prehospital-ROSC, the ROSC after cardiac arrest, Utstein-Based ROSC, and The Cardiac Arrest Survival Post-Resuscitation In-Hospital scores) were used to assess the patients. The AUROCs of the scores were compared to evaluate their diagnostic accuracy.</p><p><strong>Results: </strong>Patients were categorized into two groups based on ROSC: No-ROSC (n = 248, 75.2%) and ROSC (n = 82, 24.8%). The ROSC group had significantly more shockable rhythms (81.7% vs. 22.2%, p < 0.001) and a higher proportion of cardiac etiology (p = 0.015) compared to the No-ROSC group. The time for the ambulance to reach the patient did not significantly differ between groups (p = 0.140), but the time spent in the ambulance before arrest was significantly shorter in the ROSC group (p = 0.026). The prehospital-ROSC score had the highest diagnostic performance (AUROC 0.791), followed by The ROSC after cardiac arrest score (0.754) and The Utstein-Based ROSC score (0.716). The Cardiac Arrest Survival Post-Resuscitation In-Hospital score had the lowest performance (0.658). Prehospital-ROSC score outperformed the Utstein-Based ROSC score (p = 0.005), and the Cardiac Arrest Survival Post-Resuscitation In-Hospital score was significantly lower than both ROSC after cardiac arrest score (p = 0.031) and the prehospital-ROSC score (p < 0.001).</p><p><strong>Conclusion: </strong>Prehospital-ROSC score was the most accurate predictor of ROSC in patients experiencing cardiac arrest during ambulance transport, while the Cardiac Arrest Survival Post-Resuscitation In-Hospital score demonstrated lower predictive accuracy.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"107"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12220659/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01265-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiac arrest during ambulance transport is a complex situation that has features of both in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) but lacks a clear classification. This study aimed to evaluate the diagnostic performance of prehospital and in-hospital ROSC prediction tools in patients experiencing cardiac arrest during ambulance transport.
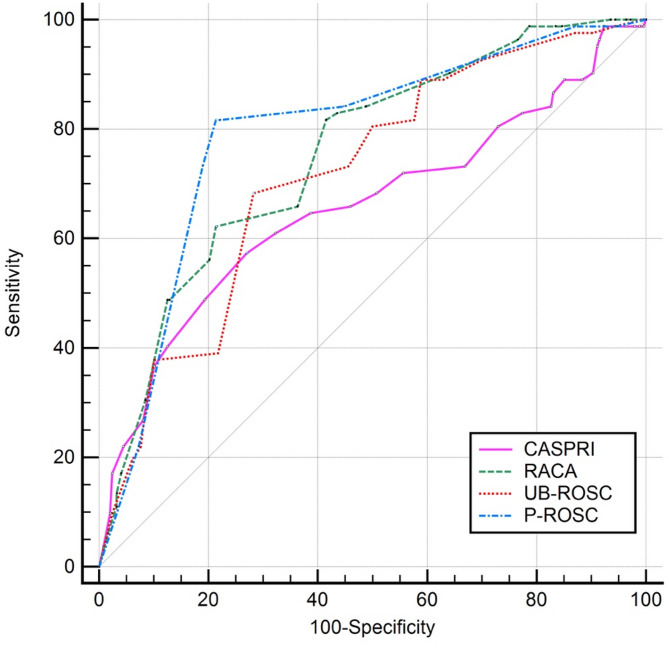
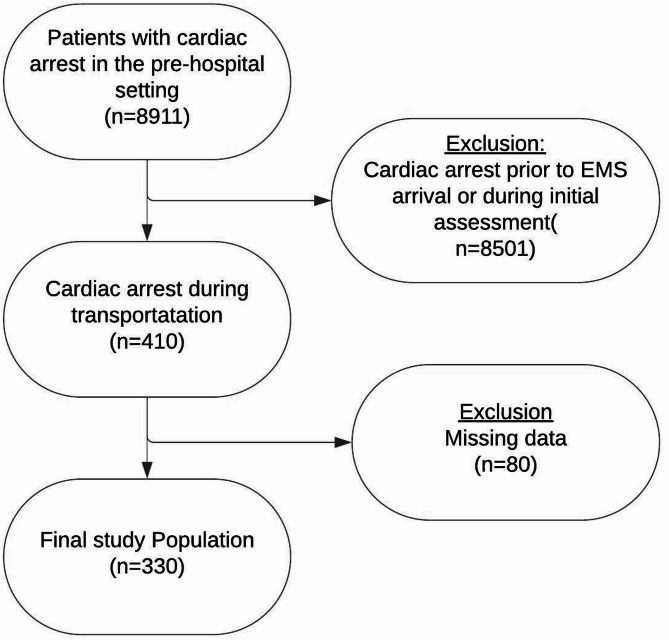
Methods: A retrospective study was conducted with patients experiencing cardiac arrest during transport. Demographic, clinical, and treatment data were collected, including pre-arrest consciousness, arrest rhythm, and cardiopulmonary resuscitation duration. Four ROSC prediction scores (Prehospital-ROSC, the ROSC after cardiac arrest, Utstein-Based ROSC, and The Cardiac Arrest Survival Post-Resuscitation In-Hospital scores) were used to assess the patients. The AUROCs of the scores were compared to evaluate their diagnostic accuracy.
Results: Patients were categorized into two groups based on ROSC: No-ROSC (n = 248, 75.2%) and ROSC (n = 82, 24.8%). The ROSC group had significantly more shockable rhythms (81.7% vs. 22.2%, p < 0.001) and a higher proportion of cardiac etiology (p = 0.015) compared to the No-ROSC group. The time for the ambulance to reach the patient did not significantly differ between groups (p = 0.140), but the time spent in the ambulance before arrest was significantly shorter in the ROSC group (p = 0.026). The prehospital-ROSC score had the highest diagnostic performance (AUROC 0.791), followed by The ROSC after cardiac arrest score (0.754) and The Utstein-Based ROSC score (0.716). The Cardiac Arrest Survival Post-Resuscitation In-Hospital score had the lowest performance (0.658). Prehospital-ROSC score outperformed the Utstein-Based ROSC score (p = 0.005), and the Cardiac Arrest Survival Post-Resuscitation In-Hospital score was significantly lower than both ROSC after cardiac arrest score (p = 0.031) and the prehospital-ROSC score (p < 0.001).
Conclusion: Prehospital-ROSC score was the most accurate predictor of ROSC in patients experiencing cardiac arrest during ambulance transport, while the Cardiac Arrest Survival Post-Resuscitation In-Hospital score demonstrated lower predictive accuracy.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


