Assessment of prehospital tracheal intubation technique using initial direct laryngoscopy during videolaryngoscopy: randomized controlled simulated trial.
{"title":"Assessment of prehospital tracheal intubation technique using initial direct laryngoscopy during videolaryngoscopy: randomized controlled simulated trial.","authors":"Cédric Cibotto, Mathieu Pasquier, Nicolas Beysard, Frédéric Rouyer, Olivier Grosgurin, Laurent Bourgeois, Elio Erriquez, Ely Braun, Birgit Andrea Gartner, Thibaut Desmettre, Laurent Suppan","doi":"10.1186/s12873-025-01266-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In critically ill patients, tracheal intubation may be required in the prehospital setting, where airway management presents unique technical and logistical challenges. While videolaryngoscopy has emerged as a potential alternative to direct laryngoscopy by providing a better and easier visualization of the glottis, the improved view of anatomical structures does not necessarily correlate with successful tracheal tube placement. Intubation may be harder because novice providers performing videolaryngoscopy may only look at the screen and only obtain a two-dimensional representation of the patient's airways. By directly visualizing the airways, these providers may obtain a better 3D apprehension and an improved mental visualization of the patient's anatomy. We compared the impact of an unrestricted videolaryngoscopy use with a sequence consisting in direct visualization of the airway followed by videolaryngoscopy (\"Direct Laryngoscopy-to-VideoLaryngoscopy sequence\" or \"DL-VL sequence\") on time to intubation among novice providers.</p><p><strong>Methods: </strong>This was a parallel group simulated randomized controlled superiority trial. Participants were medical students or junior residents with an experience of less than 10 intubations. After a presentation and workshop on direct laryngoscopy and videolaryngoscopy, participants were randomized in two groups. In the control group, participants were free to use of the videolaryngoscope as they intended. In the other group (DL-VL sequence), participants were told to perform an initial direct laryngoscopy without looking at the video screen until they reached the epiglottis. All intubations were conducted in a simulated prehospital environment, with a high-fidelity manikin placed supine on the floor. Each participant performed three intubations of increasing levels of difficulty. The primary outcome was the time to intubation. Secondary outcomes included first-pass success, time to ventilation, and number of intubation attempts. The chi-squared test was used to compare categorical variables while the t-test was used to compare continuous variables.</p><p><strong>Results: </strong>Time to intubation was shorter in the control group (22±8 s vs. 27±11 s, p < 0.001). This difference was consistent in all levels of difficulties. First-pass success rates were similar (99/111, 89% in the control group vs. 85/105, 81%, p = 0.089). Time to ventilation was significantly shorter in the control group (37±9 vs. 41±11 s, p = 0.008). The mean number of intubation attempts was similar between groups (p = 0.231).</p><p><strong>Conclusion: </strong>In this simulated study among novice providers, direct airway visualization prior to videolaryngoscopy did not improve time to intubation or to ventilation.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov, Registration Number: NCT06918717, registered on April 8th, 2025. Retrospectively registered.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"112"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12217279/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01266-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In critically ill patients, tracheal intubation may be required in the prehospital setting, where airway management presents unique technical and logistical challenges. While videolaryngoscopy has emerged as a potential alternative to direct laryngoscopy by providing a better and easier visualization of the glottis, the improved view of anatomical structures does not necessarily correlate with successful tracheal tube placement. Intubation may be harder because novice providers performing videolaryngoscopy may only look at the screen and only obtain a two-dimensional representation of the patient's airways. By directly visualizing the airways, these providers may obtain a better 3D apprehension and an improved mental visualization of the patient's anatomy. We compared the impact of an unrestricted videolaryngoscopy use with a sequence consisting in direct visualization of the airway followed by videolaryngoscopy ("Direct Laryngoscopy-to-VideoLaryngoscopy sequence" or "DL-VL sequence") on time to intubation among novice providers.
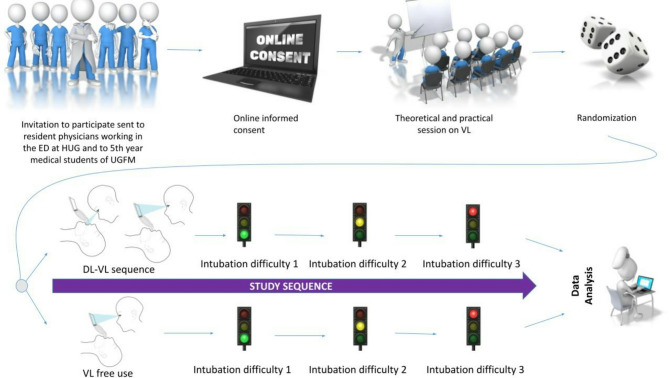
Methods: This was a parallel group simulated randomized controlled superiority trial. Participants were medical students or junior residents with an experience of less than 10 intubations. After a presentation and workshop on direct laryngoscopy and videolaryngoscopy, participants were randomized in two groups. In the control group, participants were free to use of the videolaryngoscope as they intended. In the other group (DL-VL sequence), participants were told to perform an initial direct laryngoscopy without looking at the video screen until they reached the epiglottis. All intubations were conducted in a simulated prehospital environment, with a high-fidelity manikin placed supine on the floor. Each participant performed three intubations of increasing levels of difficulty. The primary outcome was the time to intubation. Secondary outcomes included first-pass success, time to ventilation, and number of intubation attempts. The chi-squared test was used to compare categorical variables while the t-test was used to compare continuous variables.
Results: Time to intubation was shorter in the control group (22±8 s vs. 27±11 s, p < 0.001). This difference was consistent in all levels of difficulties. First-pass success rates were similar (99/111, 89% in the control group vs. 85/105, 81%, p = 0.089). Time to ventilation was significantly shorter in the control group (37±9 vs. 41±11 s, p = 0.008). The mean number of intubation attempts was similar between groups (p = 0.231).
Conclusion: In this simulated study among novice providers, direct airway visualization prior to videolaryngoscopy did not improve time to intubation or to ventilation.
Trial registration: ClinicalTrials.gov, Registration Number: NCT06918717, registered on April 8th, 2025. Retrospectively registered.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


