Patrick Tran, Mithilesh Joshi, Prithwish Banerjee, Sendhil Balasubramanian, Uday Dandekar, Emmanuel Otabor, Stephen Adeyeye, Jaffar Al-Sheikhli, Michael Kuehl
{"title":"Learning from cardiogenic shock deaths: a comparative analysis between hypotensive and normotensive cardiogenic shock.","authors":"Patrick Tran, Mithilesh Joshi, Prithwish Banerjee, Sendhil Balasubramanian, Uday Dandekar, Emmanuel Otabor, Stephen Adeyeye, Jaffar Al-Sheikhli, Michael Kuehl","doi":"10.1093/ehjopen/oeaf053","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>This study characterizes the under-recognized normotensive cardiogenic shock (CS) phenotype by analysing fatal cases, comparing haemodynamics, shock trajectories, and management gaps with hypotensive CS.</p><p><strong>Methods and results: </strong>We analysed 112 patients who died from CS between 2017 and 2022. Patients > 70 were excluded due to local eligibility criteria. Normotensive (<i>n</i> = 51) and hypotensive CS (<i>n</i> = 61) had similar degrees of cardiac impairment, with cardiac indices well below 2.0 L/min/m<sup>2</sup> and LVEF < 35%. Both groups exhibited comparable end-organ dysfunction, including lactate levels (7.0 ± 5.0 vs. 6.1 ± 5.6 mmol/L, <i>P</i> = 0.441) and acute liver injury (51-56%). Hypotensive CS typically followed a predictable decline in shock stage [75.4% deteriorated to Society for Cardiovascular Angiography Interventions (SCAI) stages D-E], whereas normotensive CS demonstrated less predictable trajectories, with 51% showing apparent stability before rapid deterioration and death. Receiver operating characteristic analysis revealed that only the rise in serum creatinine weakly predicted deterioration to advanced SCAI stages (Area under the curve 0.62, <i>P</i> = 0.035), while initial lactate and liver function tests lacked predictive value. Normotensive cases had a median 14 h longer referral window from onset of CS but were referred less frequently. Twenty-six were considered potential candidates for advanced heart failure therapy but were not referred.</p><p><strong>Conclusion: </strong>Normotensive and hypotensive CS share similar degrees of hypoperfusion but differ in their shock trajectories. The delay in referrals for normotensive CS highlights the need for earlier recognition of this phenotype and standardized protocols to ensure timely referrals for mechanical circulatory support.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf053"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12203784/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: This study characterizes the under-recognized normotensive cardiogenic shock (CS) phenotype by analysing fatal cases, comparing haemodynamics, shock trajectories, and management gaps with hypotensive CS.
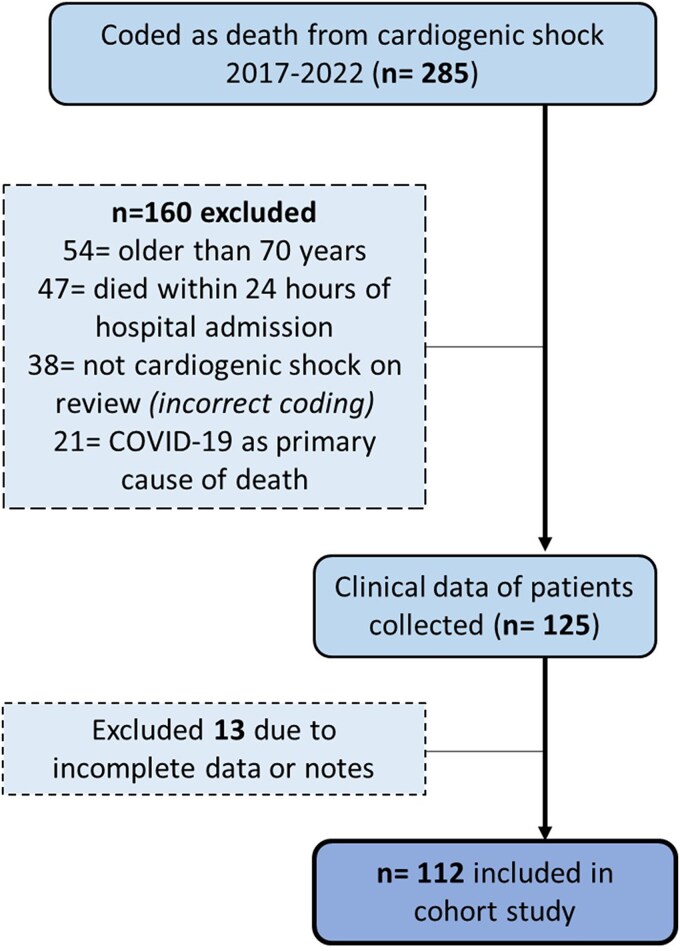
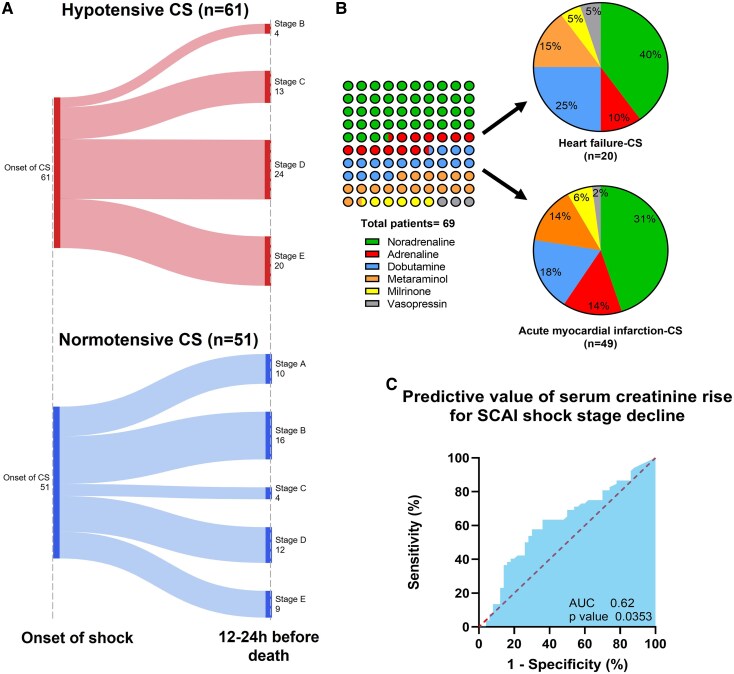
Methods and results: We analysed 112 patients who died from CS between 2017 and 2022. Patients > 70 were excluded due to local eligibility criteria. Normotensive (n = 51) and hypotensive CS (n = 61) had similar degrees of cardiac impairment, with cardiac indices well below 2.0 L/min/m2 and LVEF < 35%. Both groups exhibited comparable end-organ dysfunction, including lactate levels (7.0 ± 5.0 vs. 6.1 ± 5.6 mmol/L, P = 0.441) and acute liver injury (51-56%). Hypotensive CS typically followed a predictable decline in shock stage [75.4% deteriorated to Society for Cardiovascular Angiography Interventions (SCAI) stages D-E], whereas normotensive CS demonstrated less predictable trajectories, with 51% showing apparent stability before rapid deterioration and death. Receiver operating characteristic analysis revealed that only the rise in serum creatinine weakly predicted deterioration to advanced SCAI stages (Area under the curve 0.62, P = 0.035), while initial lactate and liver function tests lacked predictive value. Normotensive cases had a median 14 h longer referral window from onset of CS but were referred less frequently. Twenty-six were considered potential candidates for advanced heart failure therapy but were not referred.
Conclusion: Normotensive and hypotensive CS share similar degrees of hypoperfusion but differ in their shock trajectories. The delay in referrals for normotensive CS highlights the need for earlier recognition of this phenotype and standardized protocols to ensure timely referrals for mechanical circulatory support.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


