{"title":"Moving the Needle in KMT2A Rearranged Pediatric B-Cell Acute Lymphoblastic Leukemia: Newer agents and novel approaches.","authors":"Anwesha Ray, Aditi Jain, Mona Vijayaran, Steve Thomas, Jayastu Senapati, Mukul Aggarwal","doi":"10.46989/001c.141198","DOIUrl":null,"url":null,"abstract":"<p><p>Pediatric B-cell acute lymphoblastic leukemia (B-ALL) has been the poster child of progressive success in the development of leukemia therapy. Among the genomically defined high-risk subtypes of B-ALL are those with <i>KMT2A</i>-rearrangement (r) which are associated with inferior outcomes with chemotherapy-based approaches. <i>KMT2A</i>-r ALL is most common in the infantile period but can be seen beyond it and has remained a therapeutic challenge. Recent clinical trials have shown a significant improvement in response rates and survival outcomes in infantile and pediatric non-infant patients with <i>KMT2A</i>-r B-ALL when treated with blinatumomab-containing regimens. A single course of sequential blinatumomab added to Interfant-06 chemotherapy led to an exceptional improvement in 2-year disease free survival to 82% compared to 49% from historical chemotherapy only approach. In the salvage settings the use of tisagenlecleucel chimeric antigen receptor (CAR) T-cell therapy has led to high response rates and durable remissions in pediatric <i>KMT2A</i>-r B-ALL. Recently, inotuzumab ozogamicin was approved in pediatric (>1 year) relapsed/refractory B-ALL, widening immunotherapy-based salvage options. However, the efficacy of inotuzumab in <i>KMT2A</i>-r B-ALL remains questionable, given lower CD22 expression in this ALL genotype. Additionally, the approval of menin inhibitors like revumenib in <i>KMT2A</i>-r pediatric acute leukemias provides another treatment option in the salvage setting for this high-risk pediatric B-ALL subtype. These targeted agents are positively altering the treatment approaches and outcomes in pediatric <i>KMT2A</i>-r B-ALL, and the use of better residual disease monitoring with next generation sequencing might further help to refine treatment approaches in such high-risk pediatric ALL.</p>","PeriodicalId":93942,"journal":{"name":"Clinical hematology international","volume":"7 2","pages":"65-73"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12206480/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical hematology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.46989/001c.141198","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Health Professions","Score":null,"Total":0}
引用次数: 0
Abstract
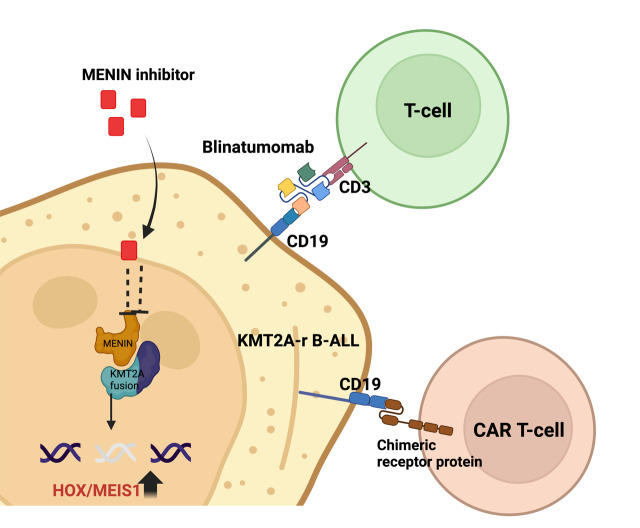
Pediatric B-cell acute lymphoblastic leukemia (B-ALL) has been the poster child of progressive success in the development of leukemia therapy. Among the genomically defined high-risk subtypes of B-ALL are those with KMT2A-rearrangement (r) which are associated with inferior outcomes with chemotherapy-based approaches. KMT2A-r ALL is most common in the infantile period but can be seen beyond it and has remained a therapeutic challenge. Recent clinical trials have shown a significant improvement in response rates and survival outcomes in infantile and pediatric non-infant patients with KMT2A-r B-ALL when treated with blinatumomab-containing regimens. A single course of sequential blinatumomab added to Interfant-06 chemotherapy led to an exceptional improvement in 2-year disease free survival to 82% compared to 49% from historical chemotherapy only approach. In the salvage settings the use of tisagenlecleucel chimeric antigen receptor (CAR) T-cell therapy has led to high response rates and durable remissions in pediatric KMT2A-r B-ALL. Recently, inotuzumab ozogamicin was approved in pediatric (>1 year) relapsed/refractory B-ALL, widening immunotherapy-based salvage options. However, the efficacy of inotuzumab in KMT2A-r B-ALL remains questionable, given lower CD22 expression in this ALL genotype. Additionally, the approval of menin inhibitors like revumenib in KMT2A-r pediatric acute leukemias provides another treatment option in the salvage setting for this high-risk pediatric B-ALL subtype. These targeted agents are positively altering the treatment approaches and outcomes in pediatric KMT2A-r B-ALL, and the use of better residual disease monitoring with next generation sequencing might further help to refine treatment approaches in such high-risk pediatric ALL.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


