{"title":"Prediction of Gastric Residual Volume by Ultrasonography in Critically Ill Children Undergoing Enteral Nutrition.","authors":"Jinjiu Hu, Qiaoying Zhang, Xin Wan, Hui Zhang, Qiao Shen, Fei Li, Ye Cai, Yuqian Meng, Peng Liu, Xianlan Zheng","doi":"10.1155/ccrp/1049746","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Bedside ultrasonography is capable of evaluating gastric residual volume (GRV) and facilitating the identification of feeding intolerance (FI) among critically ill pediatric patients; however, a specialized predictive model tailored to this demographic has yet to be established. This study aims to develop a predictive model for the estimation of GRV using ultrasonography in this specific patient group. <b>Methods:</b> This prospective observational study included critically ill pediatric patients receiving enteral nutrition (EN). Clinical data, including gender, age, weight, height, gastric antrum cross-sectional area (CSA) in supine and right lateral positions, and qualitative grading system scores (Grade 0-2), were collected. GRV was measured by suctioning gastric contents under real-time ultrasound guidance, which was considered the actual GRV. The predictive models for GRV were developed using linear regression analysis. The agreement between predicted and actual GRV values was assessed using Bland-Altman analysis. <b>Results:</b> A total of 108 children were included in the analysis. Significant differences (<i>p</i> < 0.05) were observed in GRV, GRV per kilogram, supine and right lateral decubitus (RLD) CSA among grades. Spearman correlation analysis revealed strong correlations between RLD CSA (<i>r</i> = 0.88, <i>p</i> < 0.001) and qualitative grading system scores (<i>r</i> = 0.86, <i>p</i> < 0.001) with suctioned GRV. A predictive model was developed using RLD CSA and qualitative grading system scores as predictors: GRV (mL) = -12.9 + 10.3 (RLD CSA [cm<sup>2</sup>]) + 3.3 × Grade 1 + 10.1 × Grade 2. This model demonstrated an adjusted coefficient of determination (<i>R</i> <sup>2</sup>) of 0.878, Akaike's information criterion (AIC) of 873.43, and Bayesian information criterion (BIC) of 884.06. Bland-Altman analysis showed a mean difference of 0.1 mL/kg between predicted and suctioned GRV, with 95% limits of agreement (LoA) ranging from -1.65 to 1.87 mL/kg. <b>Conclusion:</b> The results suggest that ultrasound-based monitoring can predict GRV in critically ill children. In addition, the qualitative grading system can differentiate between high and low GRV, potentially serving as a rapid screening tool for identifying patients with high GRV.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2025 ","pages":"1049746"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208764/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ccrp/1049746","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
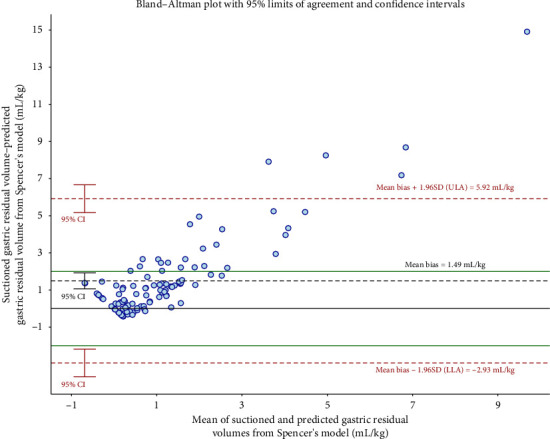
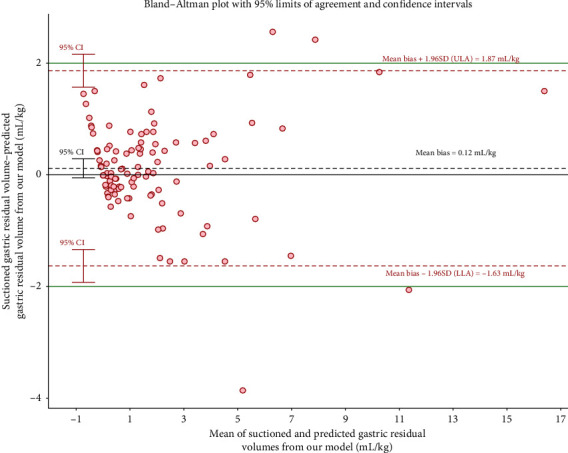
Background: Bedside ultrasonography is capable of evaluating gastric residual volume (GRV) and facilitating the identification of feeding intolerance (FI) among critically ill pediatric patients; however, a specialized predictive model tailored to this demographic has yet to be established. This study aims to develop a predictive model for the estimation of GRV using ultrasonography in this specific patient group. Methods: This prospective observational study included critically ill pediatric patients receiving enteral nutrition (EN). Clinical data, including gender, age, weight, height, gastric antrum cross-sectional area (CSA) in supine and right lateral positions, and qualitative grading system scores (Grade 0-2), were collected. GRV was measured by suctioning gastric contents under real-time ultrasound guidance, which was considered the actual GRV. The predictive models for GRV were developed using linear regression analysis. The agreement between predicted and actual GRV values was assessed using Bland-Altman analysis. Results: A total of 108 children were included in the analysis. Significant differences (p < 0.05) were observed in GRV, GRV per kilogram, supine and right lateral decubitus (RLD) CSA among grades. Spearman correlation analysis revealed strong correlations between RLD CSA (r = 0.88, p < 0.001) and qualitative grading system scores (r = 0.86, p < 0.001) with suctioned GRV. A predictive model was developed using RLD CSA and qualitative grading system scores as predictors: GRV (mL) = -12.9 + 10.3 (RLD CSA [cm2]) + 3.3 × Grade 1 + 10.1 × Grade 2. This model demonstrated an adjusted coefficient of determination (R2) of 0.878, Akaike's information criterion (AIC) of 873.43, and Bayesian information criterion (BIC) of 884.06. Bland-Altman analysis showed a mean difference of 0.1 mL/kg between predicted and suctioned GRV, with 95% limits of agreement (LoA) ranging from -1.65 to 1.87 mL/kg. Conclusion: The results suggest that ultrasound-based monitoring can predict GRV in critically ill children. In addition, the qualitative grading system can differentiate between high and low GRV, potentially serving as a rapid screening tool for identifying patients with high GRV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


