Ye In Christopher Kwon, Holly Caboti-Jones, Michael Keller, Andrew Min-Gi Park, Alan Lai, Rachit D Shah, Zachary Fitch, Vigneshwar Kasirajan, Vipul Patel, Zubair A Hashmi
{"title":"Impact of the Composite Allocation Score on Lung Transplant Waitlist and Posttransplant Outcomes.","authors":"Ye In Christopher Kwon, Holly Caboti-Jones, Michael Keller, Andrew Min-Gi Park, Alan Lai, Rachit D Shah, Zachary Fitch, Vigneshwar Kasirajan, Vipul Patel, Zubair A Hashmi","doi":"10.1097/TXD.0000000000001836","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>On March 9, 2023, the Composite Allocation Score (CAS) was introduced for all lung transplantation (LT) candidates. We analyzed waitlist and posttransplant outcomes after CAS implementation.</p><p><strong>Methods: </strong>Using the United Network for Organ Sharing registry (2022-2024), adult patients listed for isolated LT were divided into 2 eras: era 1 (pre-CAS: March 1, 2022-March 8, 2023) and era 2 (post-CAS: March 9, 2023-September 30, 2024). Competing risk regression analyzed waitlist events. Recipient/donor characteristics and mortality risk factors were assessed with Cox models. Survival was evaluated with Kaplan-Meier analysis.</p><p><strong>Results: </strong>Among 6398 LTs, 2598 (40.6%) occurred in era 2. More Black patients (16.9% versus 15%, <i>P</i> = 0.04) and those with a high school education (35.4% versus 33.4%, <i>P</i> = 0.0003) were transplanted. ABO type O patients were less likely to undergo LT (42.5% versus 46.6%, <i>P</i> = 0.04). Era 2 had longer transport distances (231 versus 202 miles, <i>P</i> < 0.0001), ischemic times (5.1 versus 4.9 h, <i>P</i> < 0.0001), and increased use of flights (79.1% versus 72.8%, <i>P</i> < 0.0001). Donation after circulatory death (9.4% versus 6.2%, <i>P</i> < 0.0001) and normothermic regional perfusion (2.2% versus 1.2%, <i>P</i> = 0.02) usage rose. Waitlist times decreased (29 versus 31 d, <i>P</i> = 0.009), with improved outcomes (sub-hazard ratio, 0.70; <i>P</i> < 0.0001). Era 2 showed superior 6-mo and 1-y survival (<i>P</i> < 0.0001) and reduced rejection treatment (2.6% versus 14.5%, <i>P</i> < 0.0001).</p><p><strong>Conclusions: </strong>The implementation of CAS was associated with reduced waitlist mortality, improved access for marginalized groups, and enhanced survival. Lungs were procured from greater distances with an increased use of donation after circulatory death with normothermic regional perfusion or ex vivo perfusion. Disparities remain for ABO type O patients, warranting closer follow-up.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 7","pages":"e1836"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208640/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001836","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: On March 9, 2023, the Composite Allocation Score (CAS) was introduced for all lung transplantation (LT) candidates. We analyzed waitlist and posttransplant outcomes after CAS implementation.
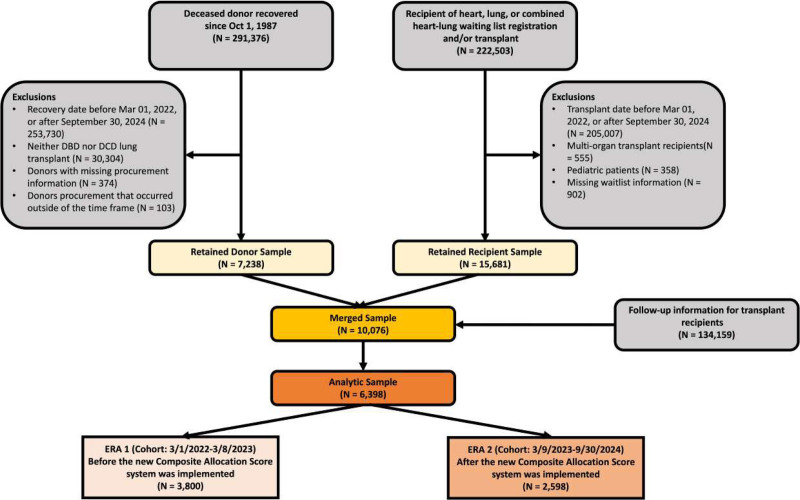
Methods: Using the United Network for Organ Sharing registry (2022-2024), adult patients listed for isolated LT were divided into 2 eras: era 1 (pre-CAS: March 1, 2022-March 8, 2023) and era 2 (post-CAS: March 9, 2023-September 30, 2024). Competing risk regression analyzed waitlist events. Recipient/donor characteristics and mortality risk factors were assessed with Cox models. Survival was evaluated with Kaplan-Meier analysis.
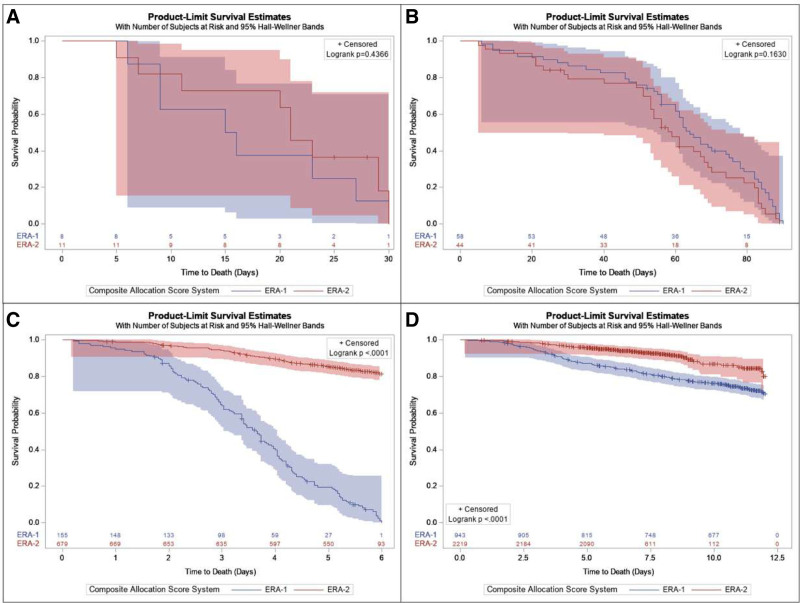
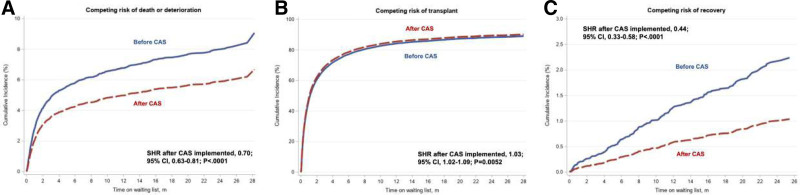
Results: Among 6398 LTs, 2598 (40.6%) occurred in era 2. More Black patients (16.9% versus 15%, P = 0.04) and those with a high school education (35.4% versus 33.4%, P = 0.0003) were transplanted. ABO type O patients were less likely to undergo LT (42.5% versus 46.6%, P = 0.04). Era 2 had longer transport distances (231 versus 202 miles, P < 0.0001), ischemic times (5.1 versus 4.9 h, P < 0.0001), and increased use of flights (79.1% versus 72.8%, P < 0.0001). Donation after circulatory death (9.4% versus 6.2%, P < 0.0001) and normothermic regional perfusion (2.2% versus 1.2%, P = 0.02) usage rose. Waitlist times decreased (29 versus 31 d, P = 0.009), with improved outcomes (sub-hazard ratio, 0.70; P < 0.0001). Era 2 showed superior 6-mo and 1-y survival (P < 0.0001) and reduced rejection treatment (2.6% versus 14.5%, P < 0.0001).
Conclusions: The implementation of CAS was associated with reduced waitlist mortality, improved access for marginalized groups, and enhanced survival. Lungs were procured from greater distances with an increased use of donation after circulatory death with normothermic regional perfusion or ex vivo perfusion. Disparities remain for ABO type O patients, warranting closer follow-up.
背景:2023年3月9日,综合分配评分(CAS)被引入所有肺移植(LT)候选人。我们分析了CAS实施后的等待名单和移植后的结果。方法:使用美国器官共享登记网络(2022-2024),将成人孤立性肝移植患者分为2个时代:第1时代(cas前:2022年3月1日至2023年3月8日)和第2时代(cas后:2023年3月9日至2024年9月30日)。竞争风险回归分析候补名单事件。采用Cox模型评估受体/供体特征和死亡危险因素。用Kaplan-Meier分析评估生存率。结果:6398例LTs中,2598例(40.6%)发生在2期。黑人患者(16.9%比15%,P = 0.04)和高中学历患者(35.4%比33.4%,P = 0.0003)接受移植较多。ABO O型患者接受LT的可能性较低(42.5%比46.6%,P = 0.04)。Era 2的运输距离更长(231英里对202英里,P P P P P = 0.02),使用率上升。等候名单时间减少(29天和31天,P = 0.009),结果改善(亚风险比,0.70;结论:CAS的实施与降低等候名单死亡率,改善边缘化群体的可及性和提高生存率有关。在循环死亡后,通过常温区域灌注或离体灌注,从更远的距离获得肺,并增加捐赠的使用。ABO O型患者的差异仍然存在,需要更密切的随访。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


