Dekel Shlomi, Michal Benderly, Liraz Olmer, Ofra Kalter-Leibovici
{"title":"Clinical and socioeconomic parameters as predictors for longer hospital stay and mortality in COPD.","authors":"Dekel Shlomi, Michal Benderly, Liraz Olmer, Ofra Kalter-Leibovici","doi":"10.1177/14799731251355445","DOIUrl":null,"url":null,"abstract":"<p><p>BackgroundIdentifying clinical and socio-economic predictors of adverse health outcomes in chronic obstructive pulmonary disease (COPD) patients is imperative for reducing exacerbation and mortality rates.MethodsThe COPD Community Disease Management (COPD-CDM) clinical trial evaluated the efficacy of a disease management program among 1202 ambulatory COPD patients receiving recommended care. The study did not find disease management to be superior to recommended care only, in preventing COPD hospital admissions or mortality. This post-hoc analysis examined the association of clinical and socioeconomic parameters with the length of in-hospital stay and all-cause mortality by multivariable non-linear mixed and Cox proportional hazards models, adjusted for age, sex, study arm, recruitment and study period, and medical therapy.ResultsA one-point increment in the Modified Medical Research Council dyspnea scale was associated with a higher hazard for all-cause mortality, (Hazards Ratio [HR]:1.50, 95% confidence interval [CI]: 1.22-1.85); longer in-hospital stay for COPD or all causes; Rate Ratio (95% CI): 1.64 (1.36-1.98), and 1.36 ( 1.19-1.55), respectively. A 50 m increment in six-minute walking distance was associated with fewer days in-hospital for both COPD and all causes; Rate Ratio (95% CI); 0.94 (0.89-0.99) and 0.95 (0.92-0.99), respectively. Unemployment and lower educational attainment were associated with a longer in-hospital stay both for COPD and all causes.ConclusionsClinical and socioeconomic parameters were associated with the number of days in hospital for COPD and all-causes, and all-cause mortality in ambulatory COPD patients. Our findings support the importance of a multi-disciplinary pulmonary approach to improve clinical outcomes among COPD patients.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":"22 ","pages":"14799731251355445"},"PeriodicalIF":2.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12206993/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731251355445","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
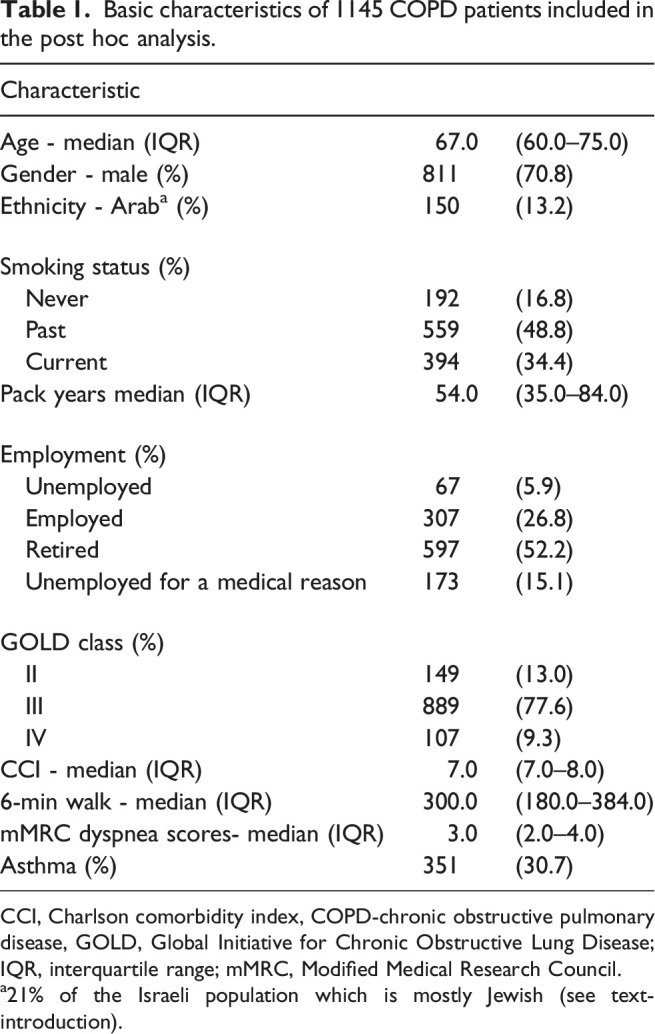
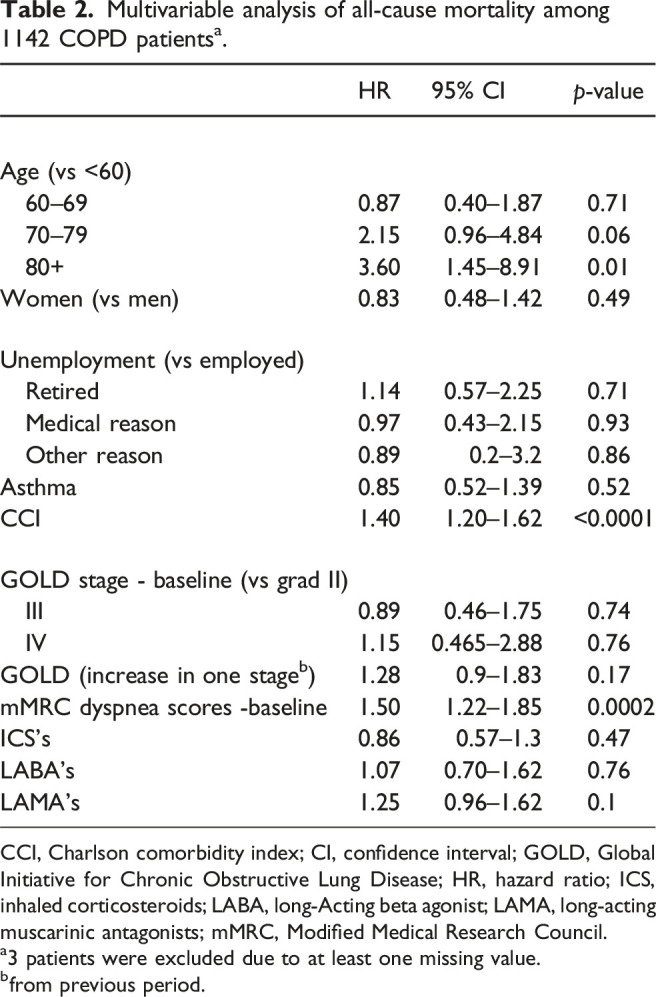
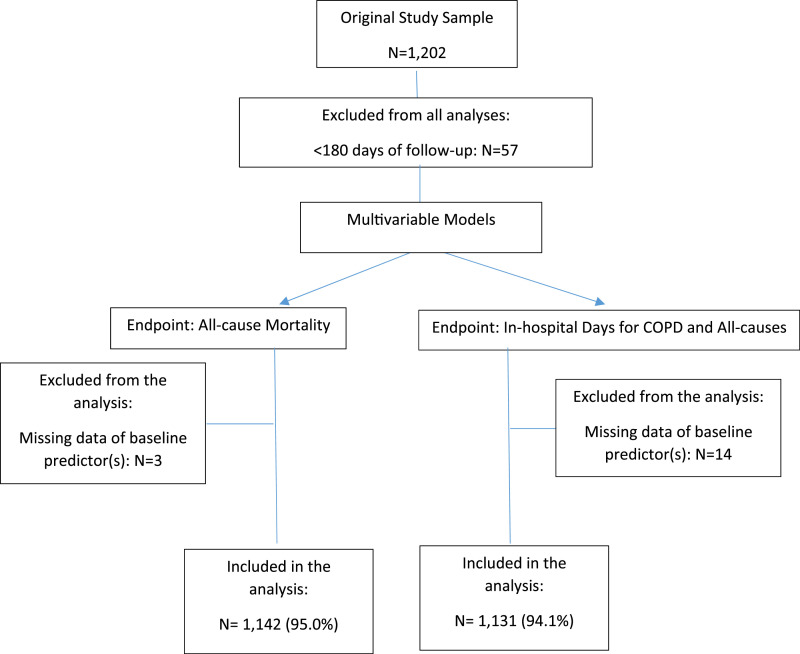
BackgroundIdentifying clinical and socio-economic predictors of adverse health outcomes in chronic obstructive pulmonary disease (COPD) patients is imperative for reducing exacerbation and mortality rates.MethodsThe COPD Community Disease Management (COPD-CDM) clinical trial evaluated the efficacy of a disease management program among 1202 ambulatory COPD patients receiving recommended care. The study did not find disease management to be superior to recommended care only, in preventing COPD hospital admissions or mortality. This post-hoc analysis examined the association of clinical and socioeconomic parameters with the length of in-hospital stay and all-cause mortality by multivariable non-linear mixed and Cox proportional hazards models, adjusted for age, sex, study arm, recruitment and study period, and medical therapy.ResultsA one-point increment in the Modified Medical Research Council dyspnea scale was associated with a higher hazard for all-cause mortality, (Hazards Ratio [HR]:1.50, 95% confidence interval [CI]: 1.22-1.85); longer in-hospital stay for COPD or all causes; Rate Ratio (95% CI): 1.64 (1.36-1.98), and 1.36 ( 1.19-1.55), respectively. A 50 m increment in six-minute walking distance was associated with fewer days in-hospital for both COPD and all causes; Rate Ratio (95% CI); 0.94 (0.89-0.99) and 0.95 (0.92-0.99), respectively. Unemployment and lower educational attainment were associated with a longer in-hospital stay both for COPD and all causes.ConclusionsClinical and socioeconomic parameters were associated with the number of days in hospital for COPD and all-causes, and all-cause mortality in ambulatory COPD patients. Our findings support the importance of a multi-disciplinary pulmonary approach to improve clinical outcomes among COPD patients.
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


