James H Seow, Damien L Stella, Christopher J Welman, Arjuna J Somasundaram, Jan F Gerstenmaier
{"title":"Washed up: the end of an era for adrenal incidentaloma CT.","authors":"James H Seow, Damien L Stella, Christopher J Welman, Arjuna J Somasundaram, Jan F Gerstenmaier","doi":"10.1186/s13244-025-02015-4","DOIUrl":null,"url":null,"abstract":"<p><p>For over 20 years, the two key tenets of adrenal incidentaloma (AI) evaluation have been the upper threshold of 10 Hounsfield units (HU) on noncontrast CT (ncCT) to delineate benignity, and the utilisation of adrenal washout CT (AWCT) to evaluate those above this cutoff. In light of growing recent evidence that challenges these two traditional principles, as well as re-evaluation of the data that led to their acceptance, we conclude that neither of these mainstays of adrenal CT remains relevant in modern AI diagnostic workup. With an appropriate definition of an incidentaloma and endocrine assessment for the majority of adrenal lesions, our analysis establishes that the use of AWCT should be ceased in the assessment of AIs, and that a 20 HU attenuation threshold for lesions < 4 cm should replace the traditional 10 HU threshold to exclude malignancy in this patient population. We therefore propose new recommendations for the management of AIs based primarily on CT attenuation and lesion size on ncCT. CRITICAL RELEVANCE STATEMENT: Increasing the CT attenuation threshold to 20 HU for lesions < 4 cm and eliminating washout CT for true adrenal incidentalomas, together with recommendations for endocrine assessment, will significantly decrease the over-investigation of overwhelmingly benign adrenal lesions, whilst confidently excluding malignancy. KEY POINTS: True incidentalomas exclude current or prior extra-adrenal malignancy and clinically suspected adrenal disease. Adrenal washout CT was never proven in the malignancy-sparse true incidentaloma population. Hormonal correlation in parallel with < 20 HU and < 4 cm thresholds of homogeneous lesions on noncontrast CT excludes malignancy.</p>","PeriodicalId":13639,"journal":{"name":"Insights into Imaging","volume":"16 1","pages":"136"},"PeriodicalIF":4.5000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204974/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Insights into Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13244-025-02015-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
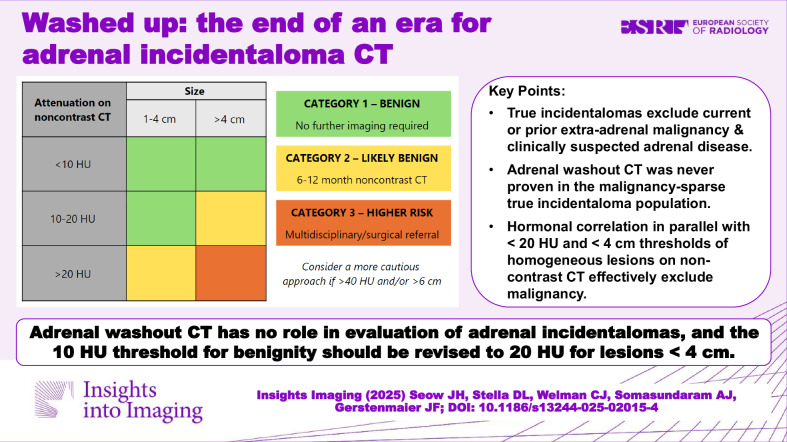
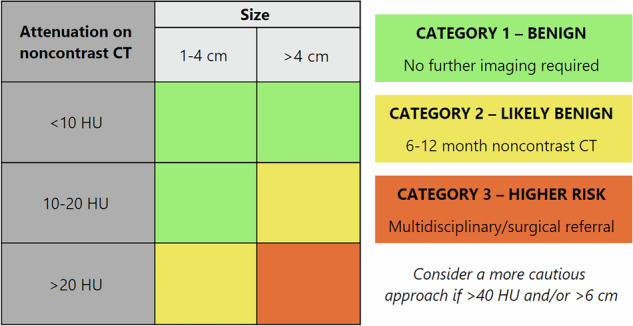
For over 20 years, the two key tenets of adrenal incidentaloma (AI) evaluation have been the upper threshold of 10 Hounsfield units (HU) on noncontrast CT (ncCT) to delineate benignity, and the utilisation of adrenal washout CT (AWCT) to evaluate those above this cutoff. In light of growing recent evidence that challenges these two traditional principles, as well as re-evaluation of the data that led to their acceptance, we conclude that neither of these mainstays of adrenal CT remains relevant in modern AI diagnostic workup. With an appropriate definition of an incidentaloma and endocrine assessment for the majority of adrenal lesions, our analysis establishes that the use of AWCT should be ceased in the assessment of AIs, and that a 20 HU attenuation threshold for lesions < 4 cm should replace the traditional 10 HU threshold to exclude malignancy in this patient population. We therefore propose new recommendations for the management of AIs based primarily on CT attenuation and lesion size on ncCT. CRITICAL RELEVANCE STATEMENT: Increasing the CT attenuation threshold to 20 HU for lesions < 4 cm and eliminating washout CT for true adrenal incidentalomas, together with recommendations for endocrine assessment, will significantly decrease the over-investigation of overwhelmingly benign adrenal lesions, whilst confidently excluding malignancy. KEY POINTS: True incidentalomas exclude current or prior extra-adrenal malignancy and clinically suspected adrenal disease. Adrenal washout CT was never proven in the malignancy-sparse true incidentaloma population. Hormonal correlation in parallel with < 20 HU and < 4 cm thresholds of homogeneous lesions on noncontrast CT excludes malignancy.
期刊介绍:
Insights into Imaging (I³) is a peer-reviewed open access journal published under the brand SpringerOpen. All content published in the journal is freely available online to anyone, anywhere!
I³ continuously updates scientific knowledge and progress in best-practice standards in radiology through the publication of original articles and state-of-the-art reviews and opinions, along with recommendations and statements from the leading radiological societies in Europe.
Founded by the European Society of Radiology (ESR), I³ creates a platform for educational material, guidelines and recommendations, and a forum for topics of controversy.
A balanced combination of review articles, original papers, short communications from European radiological congresses and information on society matters makes I³ an indispensable source for current information in this field.
I³ is owned by the ESR, however authors retain copyright to their article according to the Creative Commons Attribution License (see Copyright and License Agreement). All articles can be read, redistributed and reused for free, as long as the author of the original work is cited properly.
The open access fees (article-processing charges) for this journal are kindly sponsored by ESR for all Members.
The journal went open access in 2012, which means that all articles published since then are freely available online.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


