Julius Jelisejevas, Ali Husain, Brian Chiang, Sophie Offen, Gnalini Sathananthan, Robert Moss, Jonathon A Leipsic, Philipp Blanke, Janarthanan Sathananthan, Robert H Boone, John G Webb, David A Wood, Anson Cheung
{"title":"Late referrals and high mortality in tricuspid regurgitation: a call for timely intervention.","authors":"Julius Jelisejevas, Ali Husain, Brian Chiang, Sophie Offen, Gnalini Sathananthan, Robert Moss, Jonathon A Leipsic, Philipp Blanke, Janarthanan Sathananthan, Robert H Boone, John G Webb, David A Wood, Anson Cheung","doi":"10.1093/ehjopen/oeaf072","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Tricuspid regurgitation (TR) is associated with increased morbidity and mortality. The optimal timing for referral and intervention remains uncertain. To evaluate outcomes in patients with TR referred for tricuspid valve intervention.</p><p><strong>Methods and results: </strong>Fifty-eight consecutive patients were referred from May 2018 to April 2023. Patients were stratified into two groups: Group 1 who underwent either tricuspid valve transcatheter edge-to-edge repair (T-TEER) or transcatheter tricuspid valve replacement (TTVR); Group 2 who died without intervention due to: awaiting candidacy assessment; awaiting intervention; deemed unsuitable for intervention. Key endpoints: in-patient, 30-day, 12- and 18-month mortality; new pacemaker implantation; echocardiographic TR grading; improvement in NYHA functional class; and heart failure-related readmissions at 30 days and 12 months. Among 58 patients, 43 underwent intervention (TTVR, <i>n</i> = 29; T-TEER, <i>n</i> = 14), 15 died without intervention (awaiting assessment <i>n</i> = 11; awaiting procedure <i>n</i> = 1, unsuitable <i>n</i> = 3). At the time of referral, the mean age was 77.0 ± 9.8 years, and 52 patients (90%) were diagnosed with functional TR; 30-day mortality in Group 1 was 12%, and 12-month mortality reached 33%, with heart failure readmission (37%); 12-month mortality in Group 2 was 73%. At 18 months, mortality reached 37% in Group 1 and 100% in Group 2. Baseline characteristics differed significantly between the groups for body mass index, severity of TR (massive or torrential), NYHA III-IV symptoms, and validated mortality scores.</p><p><strong>Conclusion: </strong>Referrals for TR often occur after substantial comorbidities have developed resulting in high mortality but should be considered for a referral and intervention at an earlier stage.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf072"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12198771/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Tricuspid regurgitation (TR) is associated with increased morbidity and mortality. The optimal timing for referral and intervention remains uncertain. To evaluate outcomes in patients with TR referred for tricuspid valve intervention.
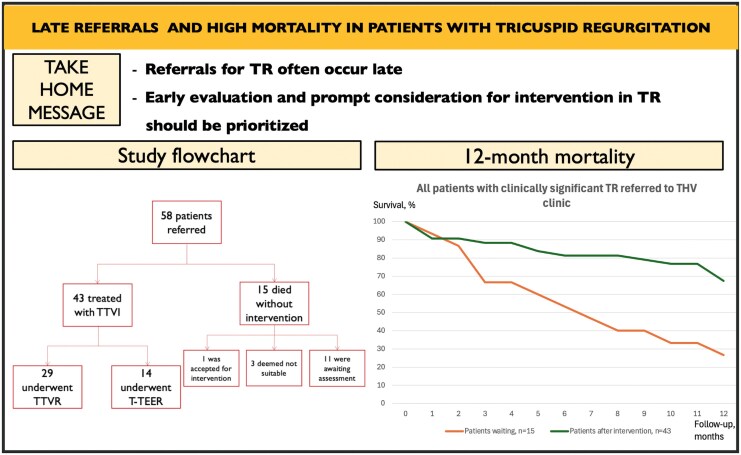
Methods and results: Fifty-eight consecutive patients were referred from May 2018 to April 2023. Patients were stratified into two groups: Group 1 who underwent either tricuspid valve transcatheter edge-to-edge repair (T-TEER) or transcatheter tricuspid valve replacement (TTVR); Group 2 who died without intervention due to: awaiting candidacy assessment; awaiting intervention; deemed unsuitable for intervention. Key endpoints: in-patient, 30-day, 12- and 18-month mortality; new pacemaker implantation; echocardiographic TR grading; improvement in NYHA functional class; and heart failure-related readmissions at 30 days and 12 months. Among 58 patients, 43 underwent intervention (TTVR, n = 29; T-TEER, n = 14), 15 died without intervention (awaiting assessment n = 11; awaiting procedure n = 1, unsuitable n = 3). At the time of referral, the mean age was 77.0 ± 9.8 years, and 52 patients (90%) were diagnosed with functional TR; 30-day mortality in Group 1 was 12%, and 12-month mortality reached 33%, with heart failure readmission (37%); 12-month mortality in Group 2 was 73%. At 18 months, mortality reached 37% in Group 1 and 100% in Group 2. Baseline characteristics differed significantly between the groups for body mass index, severity of TR (massive or torrential), NYHA III-IV symptoms, and validated mortality scores.
Conclusion: Referrals for TR often occur after substantial comorbidities have developed resulting in high mortality but should be considered for a referral and intervention at an earlier stage.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


