Two-year follow-up study (PRIMROSE 3) to assess bone mineral density in subjects with uterine fibroids completing the PRIMROSE 1 and PRIMROSE 2 linzagolix trials.
Jacques Donnez, Felice Petraglia, Hugh Taylor, Christian Becker, Sven Becker, Francisco Carmona Herrera, Maciej Paszkowski, Elke Bestel, Satoshi Hori, Marie-Madeleine Dolmans
{"title":"Two-year follow-up study (PRIMROSE 3) to assess bone mineral density in subjects with uterine fibroids completing the PRIMROSE 1 and PRIMROSE 2 linzagolix trials.","authors":"Jacques Donnez, Felice Petraglia, Hugh Taylor, Christian Becker, Sven Becker, Francisco Carmona Herrera, Maciej Paszkowski, Elke Bestel, Satoshi Hori, Marie-Madeleine Dolmans","doi":"10.1093/hropen/hoaf025","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>How important was the change in lumbar spine (L1-L4), femoral neck, and total hip bone mineral density (BMD) from post-treatment baseline values to 24 months after the end of treatment in PRIMROSE 1 and PRIMROSE 2 study participants?</p><p><strong>Summary answer: </strong>In the present study (PRIMROSE 3), mean percentage changes in lumbar spine BMD from the post-treatment baseline to month 24 (primary endpoint) were small in most treatment groups and similar to variations in the placebo group.</p><p><strong>What is known already: </strong>Due to its mechanism of action, some BMD decreases are observed with oral GnRH antagonist treatment, depending on the dose administered and addition or not of add-back therapy (ABT) (1 mg oestradiol and 0.5 mg norethisterone acetate). In PRIMROSE 1 and PRIMROSE 2, no significant changes in BMD were observed in any of the three anatomic sites investigated (lumbar spine, femoral neck, and total hip) in any of the treated groups but one. Indeed, at 24 weeks, mean differences were most pronounced in the lumbar spine in participants given 200 mg linzagolix alone.</p><p><strong>Study design size duration: </strong>PRIMROSE 3 is a long-term follow-up study on BMD in subjects who completed at least 20 weeks of treatment in the main linzagolix trials (PRIMROSE 1 or PRIMROSE 2) and underwent dual-energy X-ray absorptiometry (DEXA) within 35 days of their last treatment (week 24 or week 52 [extension study]). The primary endpoint was the change in lumbar spine (L1-L4), femoral neck, and total hip BMD from post-treatment baseline values to 24 months after the end of treatment in PRIMROSE 1 and PRIMROSE 2 study participants. The secondary endpoint was the change in lumbar spine (L1-L4), femoral neck, and total hip BMD from pre-treatment baseline values to 24 months after the end of treatment. The study involved an eligibility visit and up to three follow-up consultations at 12, 18 and/or 24 months after the end of treatment in either PRIMROSE 1 or PRIMROSE 2.</p><p><strong>Participants/materials setting methods: </strong>Patients given an end-of-treatment DEXA scan within 35 days of their last treatment were invited to participate in the PRIMROSE 3 study. Those who were pregnant or unable to undergo a DEXA scan on the same type of equipment as used for the end-of-treatment DEXA scan in PRIMROSE 1 or PRIMROSE 2 were not eligible for this trial. A total of 137 subjects were screened, 134 (97.8%) of whom were enrolled and 130 (94.9%) included in the safety analysis set. Subject groups were small and ranged from 7 subjects (placebo group) to 30 subjects (200 mg/200 mg+ABT group). Most subjects (n = 110, 80.3%) completed the study by evaluation of their BMD by DEXA at 2 years post-treatment.This study (EudraCT number: 2021-000452-19) was conducted at 3 sites in Bulgaria, 4 sites in the Czech Republic, 4 sites in Hungary, 1 site in Latvia, 6 sites in Poland, 1 site in Romania, 5 sites in Ukraine, and 32 sites in the USA.</p><p><strong>Main results and the role of chance: </strong>The most notable percentage increase from the end of treatment to month 24 was in the 200 mg/200 mg+ABT treatment group, which was also the group showing the greatest mean percentage BMD loss during linzagolix treatment. This marked upturn in BMD after cessation of treatment demonstrated the crucial role of ABT.Percentage changes in lumbar spine BMD from the pre-treatment baseline to month 24 (secondary endpoint) remained above -2% in all linzagolix treatment groups. Small BMD modifications observed from both the post-treatment and pre-treatment baseline to month 24 after the end of therapy may not have any clinically relevant impact on overall bone health of linzagolix-treated individuals, since the <i>Z</i>-score of most subjects was within the expected range for age. In addition, changes in BMD values and <i>Z</i>-scores in the linzagolix treatment groups were mostly within the same range as in the placebo group.</p><p><strong>Limitations reasons for caution: </strong>The number of patients is relatively small. Since interpretation of results from the month-12 and month-18 visits is limited due to the small number of subjects in each treatment arm at corresponding time points, giving rise to high data variability, this manuscript focuses on the month-24 visit only.</p><p><strong>Wider implications of the findings: </strong>It can be assumed that the small BMD changes observed from both the post-treatment and pre-treatment baseline to month 24 after cessation of therapy may not have any clinically relevant impact on overall bone health of linzagolix-treated individuals.Changes in BMD values and <i>Z</i>-scores in the linzagolix treatment groups were mostly within the same range as in the placebo group, indicating that there are no long-term consequences on BMD after the end of linzagolix treatment.</p><p><strong>Study funding/competing interests: </strong>Funding for the PRIMROSE studies was provided by ObsEva (Geneva, Switzerland). Analysis of data was partially supported by ObsEva (Geneva, Switzerland), Theramex (London, UK), and Kissei (Japan). Grant 5/4/150/5 was awarded to M.-M.D. by the FNRS.J.D. was a member of the scientific advisory board of ObsEva and Preglem until 2023 and reports consulting fees from ObsEva, Gedeon Richter, and Theramex. F.P. has received consulting fees and honoraria for lectures from Theramex. H.T. has received grants from Abbvie, reports consulting fees from ObsEva and Gedeon Richter, has a patent on endometriosis biomarkers owned by Yale University, and was a past president of American Society of Reproductive Medicine (ASRM). C.B. was a member of the independent data monitoring board for the PRIMROSE trials and member of the advisory board for Spirit 1 and 2 trials. He was also the Chair for the ESHRE endometriosis guideline committee. Consulting fees from Myovant and Theramex went to the University of Oxford. S.B. has received consulting fees and honoraria for lectures from Theramex. F.C.H. reports consulting fees and honoraria for lectures, presentations, or educational events from Theramex and Gedeon Richter and receiving honoraria for participation in a data safety monitoring board for Organon. M.P. was a principal investigator in the ObsEva-sponsored PRIMROSE 2 and 3 trials. E.B. and S.H. are employees of Theramex. M.-M.D. has received fees for lectures from Gedeon Richter and Theramex.</p><p><strong>Trial registration number: </strong>EudraCT number: 2021-000452-19.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 3","pages":"hoaf025"},"PeriodicalIF":11.1000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202088/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: How important was the change in lumbar spine (L1-L4), femoral neck, and total hip bone mineral density (BMD) from post-treatment baseline values to 24 months after the end of treatment in PRIMROSE 1 and PRIMROSE 2 study participants?
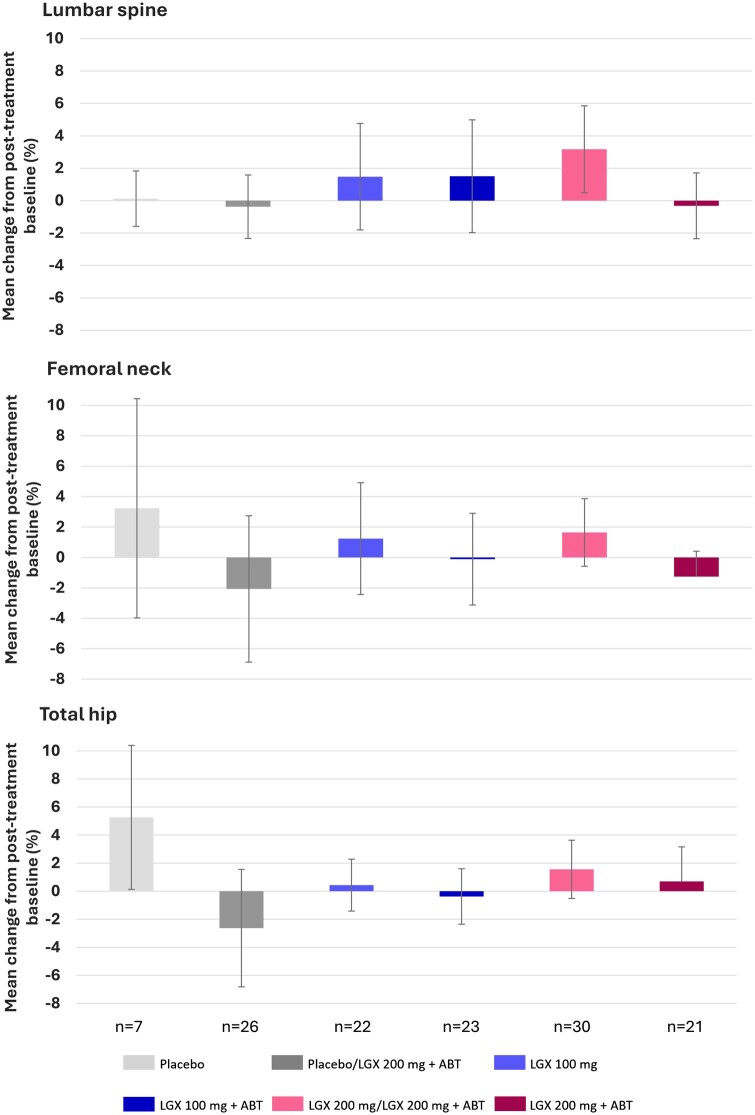
Summary answer: In the present study (PRIMROSE 3), mean percentage changes in lumbar spine BMD from the post-treatment baseline to month 24 (primary endpoint) were small in most treatment groups and similar to variations in the placebo group.
What is known already: Due to its mechanism of action, some BMD decreases are observed with oral GnRH antagonist treatment, depending on the dose administered and addition or not of add-back therapy (ABT) (1 mg oestradiol and 0.5 mg norethisterone acetate). In PRIMROSE 1 and PRIMROSE 2, no significant changes in BMD were observed in any of the three anatomic sites investigated (lumbar spine, femoral neck, and total hip) in any of the treated groups but one. Indeed, at 24 weeks, mean differences were most pronounced in the lumbar spine in participants given 200 mg linzagolix alone.
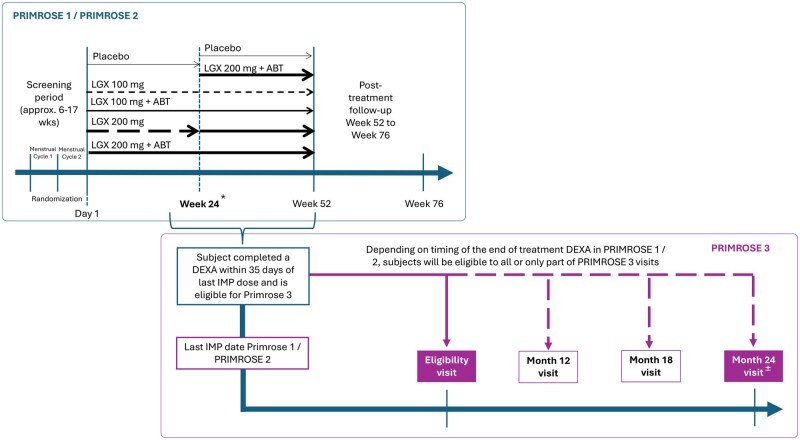
Study design size duration: PRIMROSE 3 is a long-term follow-up study on BMD in subjects who completed at least 20 weeks of treatment in the main linzagolix trials (PRIMROSE 1 or PRIMROSE 2) and underwent dual-energy X-ray absorptiometry (DEXA) within 35 days of their last treatment (week 24 or week 52 [extension study]). The primary endpoint was the change in lumbar spine (L1-L4), femoral neck, and total hip BMD from post-treatment baseline values to 24 months after the end of treatment in PRIMROSE 1 and PRIMROSE 2 study participants. The secondary endpoint was the change in lumbar spine (L1-L4), femoral neck, and total hip BMD from pre-treatment baseline values to 24 months after the end of treatment. The study involved an eligibility visit and up to three follow-up consultations at 12, 18 and/or 24 months after the end of treatment in either PRIMROSE 1 or PRIMROSE 2.
Participants/materials setting methods: Patients given an end-of-treatment DEXA scan within 35 days of their last treatment were invited to participate in the PRIMROSE 3 study. Those who were pregnant or unable to undergo a DEXA scan on the same type of equipment as used for the end-of-treatment DEXA scan in PRIMROSE 1 or PRIMROSE 2 were not eligible for this trial. A total of 137 subjects were screened, 134 (97.8%) of whom were enrolled and 130 (94.9%) included in the safety analysis set. Subject groups were small and ranged from 7 subjects (placebo group) to 30 subjects (200 mg/200 mg+ABT group). Most subjects (n = 110, 80.3%) completed the study by evaluation of their BMD by DEXA at 2 years post-treatment.This study (EudraCT number: 2021-000452-19) was conducted at 3 sites in Bulgaria, 4 sites in the Czech Republic, 4 sites in Hungary, 1 site in Latvia, 6 sites in Poland, 1 site in Romania, 5 sites in Ukraine, and 32 sites in the USA.
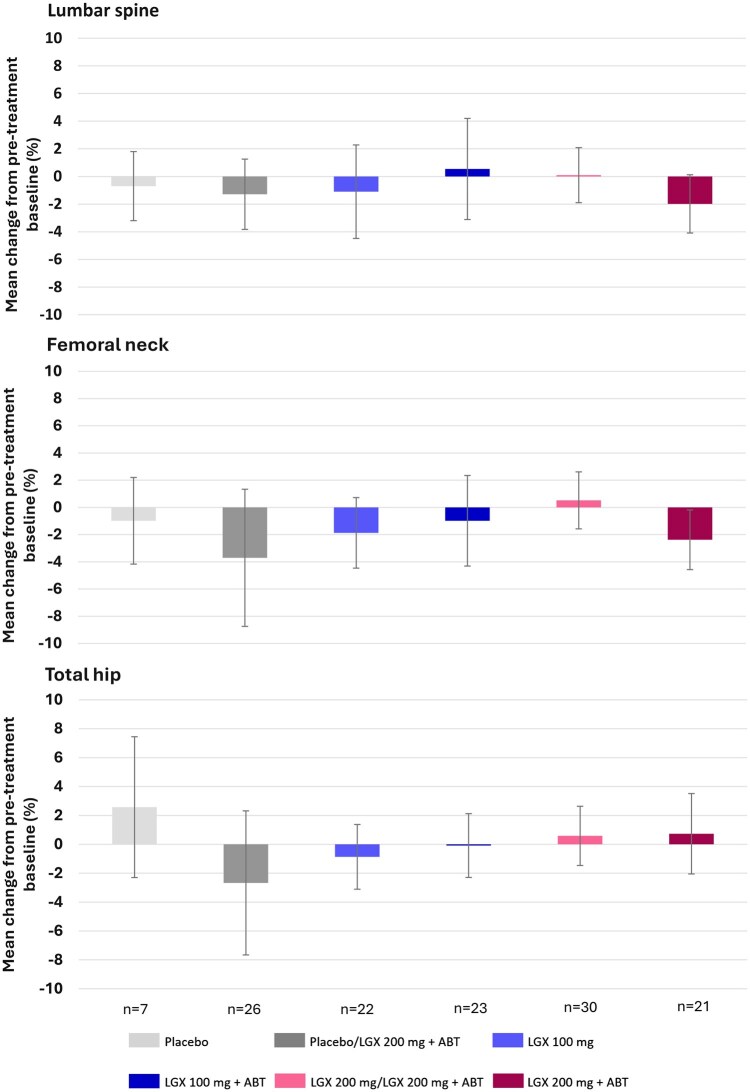
Main results and the role of chance: The most notable percentage increase from the end of treatment to month 24 was in the 200 mg/200 mg+ABT treatment group, which was also the group showing the greatest mean percentage BMD loss during linzagolix treatment. This marked upturn in BMD after cessation of treatment demonstrated the crucial role of ABT.Percentage changes in lumbar spine BMD from the pre-treatment baseline to month 24 (secondary endpoint) remained above -2% in all linzagolix treatment groups. Small BMD modifications observed from both the post-treatment and pre-treatment baseline to month 24 after the end of therapy may not have any clinically relevant impact on overall bone health of linzagolix-treated individuals, since the Z-score of most subjects was within the expected range for age. In addition, changes in BMD values and Z-scores in the linzagolix treatment groups were mostly within the same range as in the placebo group.
Limitations reasons for caution: The number of patients is relatively small. Since interpretation of results from the month-12 and month-18 visits is limited due to the small number of subjects in each treatment arm at corresponding time points, giving rise to high data variability, this manuscript focuses on the month-24 visit only.
Wider implications of the findings: It can be assumed that the small BMD changes observed from both the post-treatment and pre-treatment baseline to month 24 after cessation of therapy may not have any clinically relevant impact on overall bone health of linzagolix-treated individuals.Changes in BMD values and Z-scores in the linzagolix treatment groups were mostly within the same range as in the placebo group, indicating that there are no long-term consequences on BMD after the end of linzagolix treatment.
Study funding/competing interests: Funding for the PRIMROSE studies was provided by ObsEva (Geneva, Switzerland). Analysis of data was partially supported by ObsEva (Geneva, Switzerland), Theramex (London, UK), and Kissei (Japan). Grant 5/4/150/5 was awarded to M.-M.D. by the FNRS.J.D. was a member of the scientific advisory board of ObsEva and Preglem until 2023 and reports consulting fees from ObsEva, Gedeon Richter, and Theramex. F.P. has received consulting fees and honoraria for lectures from Theramex. H.T. has received grants from Abbvie, reports consulting fees from ObsEva and Gedeon Richter, has a patent on endometriosis biomarkers owned by Yale University, and was a past president of American Society of Reproductive Medicine (ASRM). C.B. was a member of the independent data monitoring board for the PRIMROSE trials and member of the advisory board for Spirit 1 and 2 trials. He was also the Chair for the ESHRE endometriosis guideline committee. Consulting fees from Myovant and Theramex went to the University of Oxford. S.B. has received consulting fees and honoraria for lectures from Theramex. F.C.H. reports consulting fees and honoraria for lectures, presentations, or educational events from Theramex and Gedeon Richter and receiving honoraria for participation in a data safety monitoring board for Organon. M.P. was a principal investigator in the ObsEva-sponsored PRIMROSE 2 and 3 trials. E.B. and S.H. are employees of Theramex. M.-M.D. has received fees for lectures from Gedeon Richter and Theramex.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


