Anik R Patel, Bradley Kievit, Ken Hasegawa, Markqayne Ray, Rishika Sharma, Sarahmaria Hofmann, Rob Blissett, Frederick L Locke
{"title":"A Cost-Effectiveness Analysis of Diffuse Large B-Cell Lymphoma Treatment Pathways in the United States.","authors":"Anik R Patel, Bradley Kievit, Ken Hasegawa, Markqayne Ray, Rishika Sharma, Sarahmaria Hofmann, Rob Blissett, Frederick L Locke","doi":"10.1177/23814683251345780","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background.</b> Chimeric antigen receptor (CAR) T-cell therapies are approved as second-line (2L) or later therapy for diffuse large B-cell lymphoma (DLBCL). Recently, bispecific T-cell antibodies (BsAbs) have been approved as third-line (3L) treatments. The cost-effectiveness of different treatment sequences is unknown. This study aims to evaluate the cost-effectiveness of axicabtagene ciloleucel (axi-cel) compared with other treatment options for 2L DLBCL, from a US health care perspective at a cost-effectiveness threshold of $150,000 per quality-adjusted life-year (QALY). <b>Design.</b> This economic evaluation used a discrete event simulation decision. Model inputs were derived from 8 clinical trials and the published literature. Simulated patients received 2L axi-cel followed by 3L treatments, which were compared with treatment sequences of 2L intended autologous stem cell transplant (ASCT), polatuzumab vedotin with bendamustine and rituximab (Pola-BR), tafasitamab with lenalidomide (tafa-len), or rituximab with gemcitabine and oxaliplatin (R-GemOx), all of which were followed by 3L treatments (salvage chemotherapy, BsAbs, or axi-cel). In addition, axi-cel was compared directly with glofitamab and epcoritamab in 3L. Costs and QALYs, discounted at 3.0%, were used to derive incremental cost-effectiveness ratios (ICERs) and net monetary benefits (NMBs). <b>Results.</b> In the 2L base case, axi-cel was cost-effective compared with intended ASCT (ICER $145,004/QALY), which was cost-effective compared with R-GemOx (ICER $9,495/QALY). Axi-cel maximized NMB at $150,000 and $200,000/QALY thresholds, whereas intended ASCT maximized NMB at $100,000/QALY. In 3L-focused comparisons with epcoritamab and glofitamab, axi-cel was dominant and cost-effective (ICER $122,224/QALY), respectively. Axi-cel maximized NMB at $150,000 and $200,000/QALY thresholds, whereas glofitamab maximized NMB at $100,000/QALY. <b>Conclusions.</b> The findings of the study suggest that although other treatments were cost-effective at lower thresholds, axi-cel is a cost-effective treatment option in 2L/3L settings in the United States.</p><p><strong>Highlights: </strong>This study investigated whether axicabtagene ciloleucel (axi-cel) is cost-effective in second-line (2L) and third-line (3L) treatment sequences in the current relapsed or refractory (R/R) diffuse large B-cell lymphoma (DLBCL) treatment paradigm.Using a novel treatment sequencing model, axi-cel was found to be cost-effective in both 2L treatment sequences and in direct comparisons with 3L bispecific T-cell antibodies.These findings suggest that axi-cel is a cost-effective treatment for R/R DLBCL regardless of treatment line positioning.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"10 1","pages":"23814683251345780"},"PeriodicalIF":1.7000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12198509/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683251345780","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
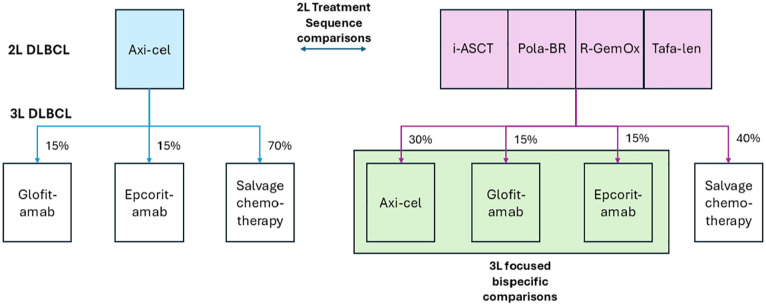
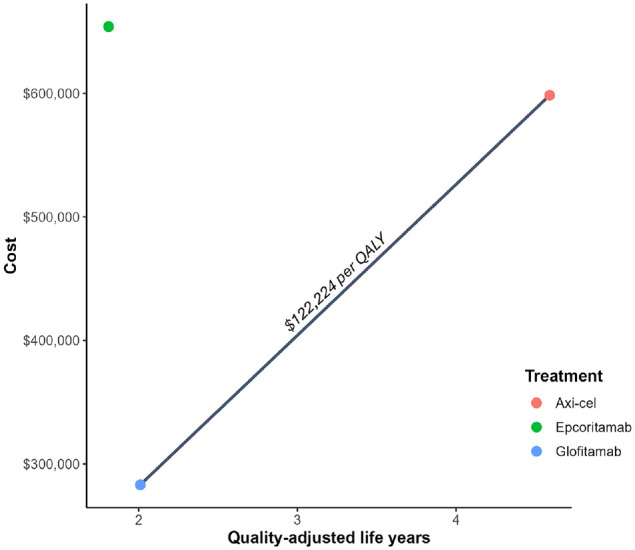
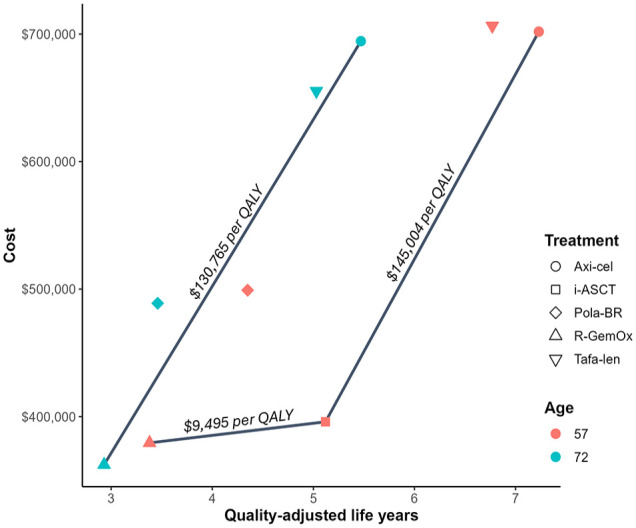
Background. Chimeric antigen receptor (CAR) T-cell therapies are approved as second-line (2L) or later therapy for diffuse large B-cell lymphoma (DLBCL). Recently, bispecific T-cell antibodies (BsAbs) have been approved as third-line (3L) treatments. The cost-effectiveness of different treatment sequences is unknown. This study aims to evaluate the cost-effectiveness of axicabtagene ciloleucel (axi-cel) compared with other treatment options for 2L DLBCL, from a US health care perspective at a cost-effectiveness threshold of $150,000 per quality-adjusted life-year (QALY). Design. This economic evaluation used a discrete event simulation decision. Model inputs were derived from 8 clinical trials and the published literature. Simulated patients received 2L axi-cel followed by 3L treatments, which were compared with treatment sequences of 2L intended autologous stem cell transplant (ASCT), polatuzumab vedotin with bendamustine and rituximab (Pola-BR), tafasitamab with lenalidomide (tafa-len), or rituximab with gemcitabine and oxaliplatin (R-GemOx), all of which were followed by 3L treatments (salvage chemotherapy, BsAbs, or axi-cel). In addition, axi-cel was compared directly with glofitamab and epcoritamab in 3L. Costs and QALYs, discounted at 3.0%, were used to derive incremental cost-effectiveness ratios (ICERs) and net monetary benefits (NMBs). Results. In the 2L base case, axi-cel was cost-effective compared with intended ASCT (ICER $145,004/QALY), which was cost-effective compared with R-GemOx (ICER $9,495/QALY). Axi-cel maximized NMB at $150,000 and $200,000/QALY thresholds, whereas intended ASCT maximized NMB at $100,000/QALY. In 3L-focused comparisons with epcoritamab and glofitamab, axi-cel was dominant and cost-effective (ICER $122,224/QALY), respectively. Axi-cel maximized NMB at $150,000 and $200,000/QALY thresholds, whereas glofitamab maximized NMB at $100,000/QALY. Conclusions. The findings of the study suggest that although other treatments were cost-effective at lower thresholds, axi-cel is a cost-effective treatment option in 2L/3L settings in the United States.
Highlights: This study investigated whether axicabtagene ciloleucel (axi-cel) is cost-effective in second-line (2L) and third-line (3L) treatment sequences in the current relapsed or refractory (R/R) diffuse large B-cell lymphoma (DLBCL) treatment paradigm.Using a novel treatment sequencing model, axi-cel was found to be cost-effective in both 2L treatment sequences and in direct comparisons with 3L bispecific T-cell antibodies.These findings suggest that axi-cel is a cost-effective treatment for R/R DLBCL regardless of treatment line positioning.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


