{"title":"Endovascular management of intermediate-risk pulmonary embolism: evidence, outstanding questions, drivers of utilization, and the horizon.","authors":"Arman A Shahriar, Jonathan Paul, Adam Cifu","doi":"10.1093/ehjopen/oeaf071","DOIUrl":null,"url":null,"abstract":"<p><p>In patients with acute intermediate-risk pulmonary embolism (PE) guidelines recommend systemic anticoagulation (Class I; Level A), but intermediate-risk patients are increasingly being treated with adjunctive endovascular (catheter-based) therapies. This review defines outstanding clinical questions, contextualizes completed and ongoing clinical studies, examines plausible drivers of utilization, and anticipates scenarios on the horizon for endovascular therapy in this large and heterogenous subgroup of patients. In intermediate-risk PE, up-front adjunctive systemic thrombolysis reduces haemodynamic deterioration or death, but the small benefit is outweighed by the risk of major bleeding. Endovascular modalities (e.g. ultrasound-assisted catheter directed thrombolysis, mechanical thrombectomy) aim to uphold these benefits while improving upon safety. Since 2014, five devices have entered the market based primarily on single-arm studies demonstrating short-term improvements in surrogate markers of effectiveness (e.g. 48 h reduction in RV/LV ratio). While thousands of patients with intermediate-risk PE (primarily intermediate-<i>high</i> risk PE) have been enrolled in prospective studies using these devices, only three small Randomized controlled trials (RCTs) have compared adjunctive endovascular therapy with anticoagulation alone, and none have included patient-centred efficacy endpoints (i.e. mortality or morbidity). In the absence of high-quality evidence or guideline recommendations, rising utilization in intermediate-risk patients may be driven by clinical uncertainty, PE response teams, favourable regulation and reimbursement, industry marketing, and financial incentives for various stakeholders. Three large RCTs are currently enrolling patients to evaluate both short- and long-term patient-centred measures of efficacy as well as safety of adjunct endovascular therapy relative to anticoagulation alone. The results of these trials will provide critical insights by the decade's end.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf071"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12188119/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
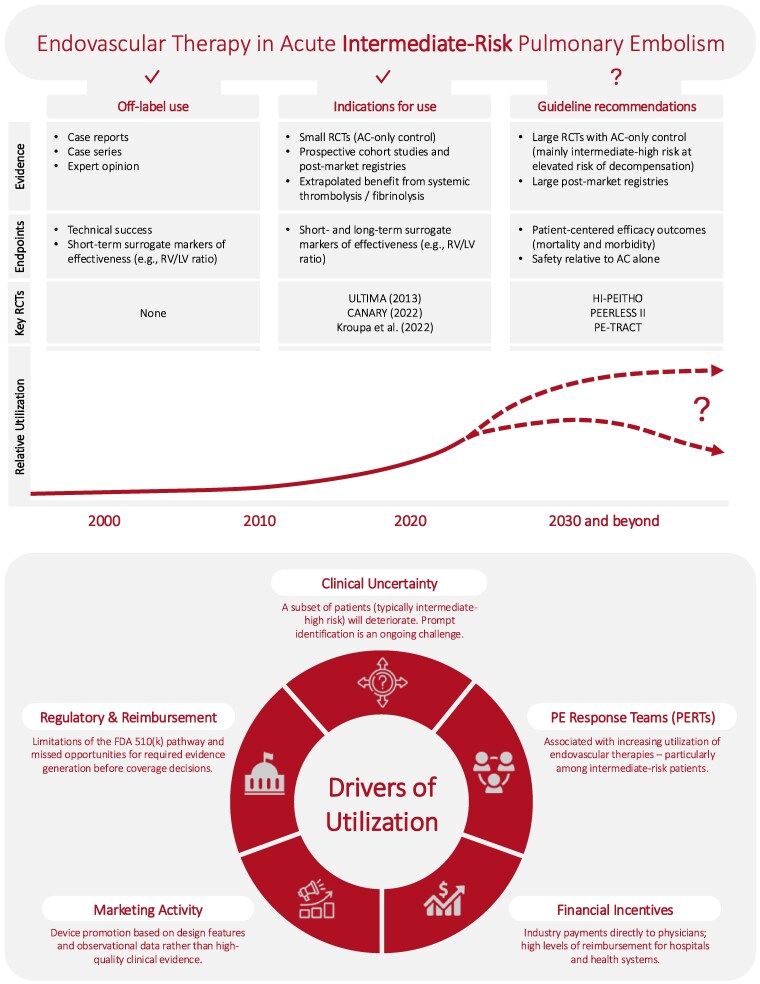
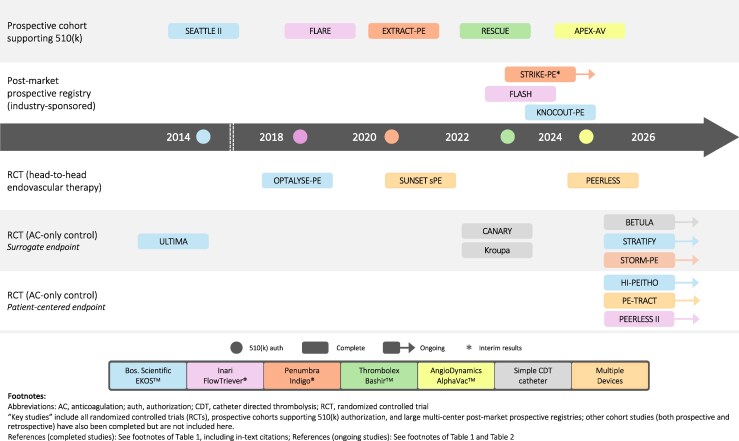
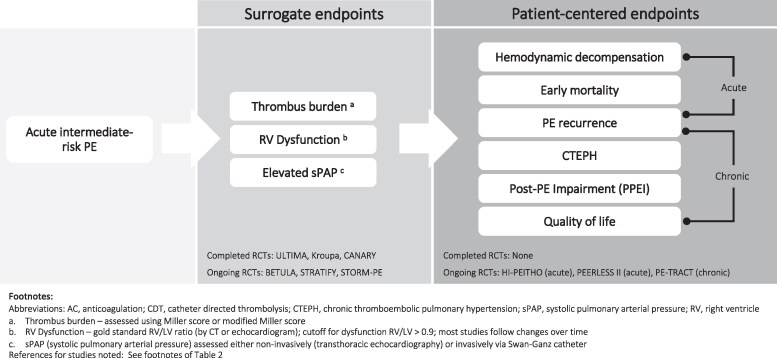
In patients with acute intermediate-risk pulmonary embolism (PE) guidelines recommend systemic anticoagulation (Class I; Level A), but intermediate-risk patients are increasingly being treated with adjunctive endovascular (catheter-based) therapies. This review defines outstanding clinical questions, contextualizes completed and ongoing clinical studies, examines plausible drivers of utilization, and anticipates scenarios on the horizon for endovascular therapy in this large and heterogenous subgroup of patients. In intermediate-risk PE, up-front adjunctive systemic thrombolysis reduces haemodynamic deterioration or death, but the small benefit is outweighed by the risk of major bleeding. Endovascular modalities (e.g. ultrasound-assisted catheter directed thrombolysis, mechanical thrombectomy) aim to uphold these benefits while improving upon safety. Since 2014, five devices have entered the market based primarily on single-arm studies demonstrating short-term improvements in surrogate markers of effectiveness (e.g. 48 h reduction in RV/LV ratio). While thousands of patients with intermediate-risk PE (primarily intermediate-high risk PE) have been enrolled in prospective studies using these devices, only three small Randomized controlled trials (RCTs) have compared adjunctive endovascular therapy with anticoagulation alone, and none have included patient-centred efficacy endpoints (i.e. mortality or morbidity). In the absence of high-quality evidence or guideline recommendations, rising utilization in intermediate-risk patients may be driven by clinical uncertainty, PE response teams, favourable regulation and reimbursement, industry marketing, and financial incentives for various stakeholders. Three large RCTs are currently enrolling patients to evaluate both short- and long-term patient-centred measures of efficacy as well as safety of adjunct endovascular therapy relative to anticoagulation alone. The results of these trials will provide critical insights by the decade's end.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


