Davide De Marco, Valerie Heron, Alain Bitton, Talat Bessissow, Peter Lakatos, Gary Wild, Waqqas Afif
{"title":"Assessing the role of ustekinumab dose escalation in Crohn's disease patients with loss of response: an observational study.","authors":"Davide De Marco, Valerie Heron, Alain Bitton, Talat Bessissow, Peter Lakatos, Gary Wild, Waqqas Afif","doi":"10.1093/jcag/gwaf001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>Among Crohn's disease patients with loss of response or non-response to ustekinumab (UST), there remains no clear strategy for dose escalation. Moreover, clinical associations and the role of therapeutic drug monitoring (TDM) are poorly understood. This study assessed response to escalation of UST therapy via increased dosing frequency or re-induction, as well as assessed associations of response.</p><p><strong>Methods: </strong>A single-centre retrospective cohort study was performed. Adults who underwent dose escalation to every 4 weeks or reinduction of UST were included. The primary outcome was clinical and biochemical remission which was defined as a Harvey Bradshaw Index (HBI) of <5 and a C-reactive protein (CRP) level within the normal limit or a Fecal Calprotectin (FCP) level <250 ug/g. Partial response to treatment was defined as a 50% decrease from baseline HBI, CRP, or FCP.</p><p><strong>Results: </strong>Thirty-nine patients were included. Clinical outcomes were assessed at a median of 17 weeks (IQR 12-21). Clinical and biochemical remission was achieved in 30.8% of patients (<i>n</i> = 12). Remission was found to be more likely among patients with lower baseline HBI (5.2 vs 9.0 <i>P</i> = .044) and younger patients (29.8 years vs 37.7 <i>P</i> = .046). No association was observed between baseline TDM values in the remission vs the non-remission group (3.32 ug/mL vs 2.91 ug/mL p=0.77). No severe adverse events were recorded.</p><p><strong>Conclusion: </strong>UST dose escalation, in the form of reinduction or increased frequency to every 4 weeks may be effective among patients with loss of response or partial response, though predictors of response and strategy of escalation remain unclear.</p>","PeriodicalId":17263,"journal":{"name":"Journal of the Canadian Association of Gastroenterology","volume":"8 3","pages":"97-102"},"PeriodicalIF":2.7000,"publicationDate":"2025-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12192420/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Canadian Association of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jcag/gwaf001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aims: Among Crohn's disease patients with loss of response or non-response to ustekinumab (UST), there remains no clear strategy for dose escalation. Moreover, clinical associations and the role of therapeutic drug monitoring (TDM) are poorly understood. This study assessed response to escalation of UST therapy via increased dosing frequency or re-induction, as well as assessed associations of response.
Methods: A single-centre retrospective cohort study was performed. Adults who underwent dose escalation to every 4 weeks or reinduction of UST were included. The primary outcome was clinical and biochemical remission which was defined as a Harvey Bradshaw Index (HBI) of <5 and a C-reactive protein (CRP) level within the normal limit or a Fecal Calprotectin (FCP) level <250 ug/g. Partial response to treatment was defined as a 50% decrease from baseline HBI, CRP, or FCP.
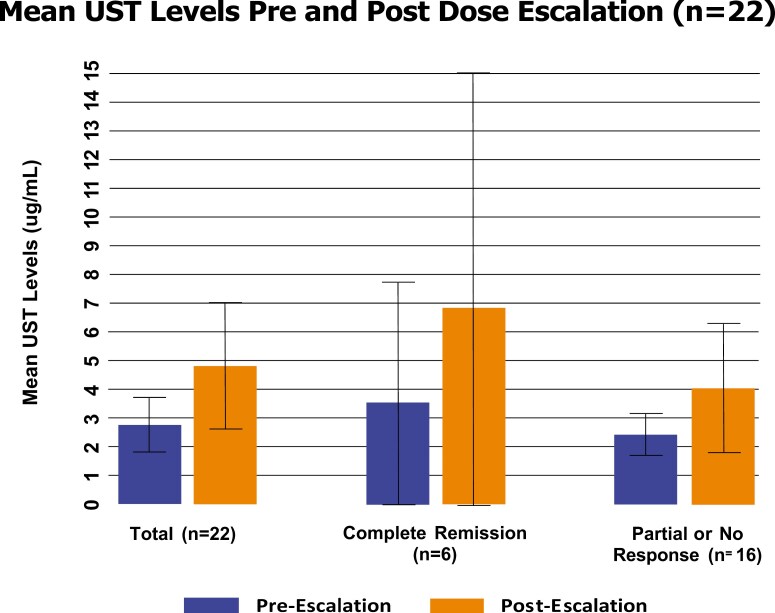
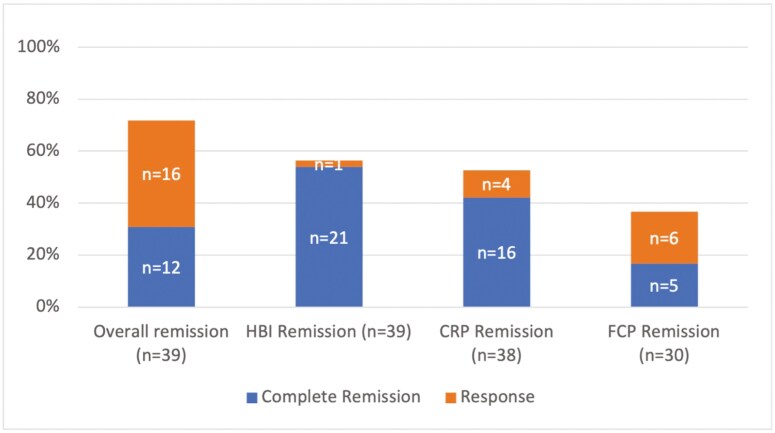
Results: Thirty-nine patients were included. Clinical outcomes were assessed at a median of 17 weeks (IQR 12-21). Clinical and biochemical remission was achieved in 30.8% of patients (n = 12). Remission was found to be more likely among patients with lower baseline HBI (5.2 vs 9.0 P = .044) and younger patients (29.8 years vs 37.7 P = .046). No association was observed between baseline TDM values in the remission vs the non-remission group (3.32 ug/mL vs 2.91 ug/mL p=0.77). No severe adverse events were recorded.
Conclusion: UST dose escalation, in the form of reinduction or increased frequency to every 4 weeks may be effective among patients with loss of response or partial response, though predictors of response and strategy of escalation remain unclear.
背景/目的:在对ustekinumab (UST)失去反应或无反应的克罗恩病患者中,仍然没有明确的剂量递增策略。此外,临床关联和治疗药物监测(TDM)的作用了解甚少。本研究通过增加给药频率或再诱导来评估对UST治疗升级的反应,以及评估反应的相关性。方法:采用单中心回顾性队列研究。接受剂量增加至每4周一次或再次诱导UST的成人纳入研究。主要结局是临床和生化缓解,定义为哈维布拉德肖指数(HBI)的结果:39例患者纳入。临床结果评估的中位时间为17周(IQR 12-21)。30.8%的患者(n = 12)达到临床和生化缓解。基线HBI较低的患者(5.2 vs 9.0 P = 0.044)和较年轻的患者(29.8 vs 37.7 P = 0.046)更容易出现缓解。缓解组和非缓解组的基线TDM值之间没有关联(3.32 ug/mL vs 2.91 ug/mL p=0.77)。无严重不良事件记录。结论:对于丧失反应或部分反应的患者,以再诱导或频率增加至每4周的形式增加UST剂量可能是有效的,尽管反应的预测因素和增加剂量的策略尚不清楚。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


