K. Furrer MD , D. Bettex MD , T. Horisberger , I. Inci MD , N.G. Nagaraj , H.-T. Morselli , B. Battilana , R. Schuepbach MD , S. Ulrich MD , M. Hebeisen MSc , I. Opitz MD
{"title":"Fluid management of cardiopulmonary bypass during pulmonary endarterectomy for CTEPH patients impacts perioperative outcome","authors":"K. Furrer MD , D. Bettex MD , T. Horisberger , I. Inci MD , N.G. Nagaraj , H.-T. Morselli , B. Battilana , R. Schuepbach MD , S. Ulrich MD , M. Hebeisen MSc , I. Opitz MD","doi":"10.1016/j.jhlto.2025.100253","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Pulmonary endarterectomy (PEA) using deep hypothermic circulatory arrest (DHCA) and cardiopulmonary bypass (CPB) is the preferred treatment for chronic thromboembolic pulmonary hypertension (CTEPH). Crystalloid priming solutions cause hemodilution with disadvantages, and no standard exists for PEA. This study evaluates CTEPH patient outcomes after adding 5% human albumin (HA) to the CPB-prime and hemodilution solution during PEA.</div></div><div><h3>Methods</h3><div>The effect of the CPB-protocol change was evaluated by comparing patients operated under the old and new protocols in a 1:1 propensity score match based on age, sex, and preoperative peripheral vascular resistance (PVR).</div></div><div><h3>Results</h3><div>Matching resulted in 56 patients (28 per group) between July 1, 2010, and May 31, 2020. The new protocol group had a lower intraoperative fluid balance (1.85 vs 6.76 liters, <em>p</em> < 0.001), vasoactive-inotropic score (VIS) (8.7 vs 17.7, <em>p</em> = 0.04), shorter operative- (407 vs 451 min, <em>p</em> = 0.03), and hospitalization time (LOS) (18 vs 27 days, <em>p</em> = 0.008). Morbidity and mortality at 30- and 90-days were similar in both groups. The new protocol was associated with reduced intraoperative fluid balance after adjustment for operative time (−3.7 liters [95% CI −5.2, −2.1], <em>p</em> < 0.0001). Lower intraoperative fluid balance was associated with shorter hospitalization in the intensive care unit, intubation time, LOS, and lower VIS (<em>p</em> = 0.0011, 0.0013, 0.008, <0.0001, respectively). The protocol change shortened LOS, independent of operative time, by 27% [95% CI, 44%, 6%], <em>p</em> = 0.02.</div></div><div><h3>Conclusions</h3><div>Priming and maintenance protocol for CPB with the addition of 5% HA had a beneficial effect on intraoperative fluid balance and improved outcome after PEA for patients with CTEPH.</div></div>","PeriodicalId":100741,"journal":{"name":"JHLT Open","volume":"9 ","pages":"Article 100253"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHLT Open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2950133425000485","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
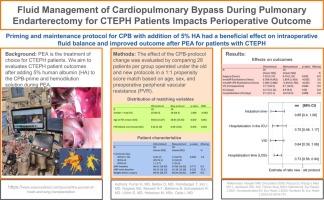
Pulmonary endarterectomy (PEA) using deep hypothermic circulatory arrest (DHCA) and cardiopulmonary bypass (CPB) is the preferred treatment for chronic thromboembolic pulmonary hypertension (CTEPH). Crystalloid priming solutions cause hemodilution with disadvantages, and no standard exists for PEA. This study evaluates CTEPH patient outcomes after adding 5% human albumin (HA) to the CPB-prime and hemodilution solution during PEA.
Methods
The effect of the CPB-protocol change was evaluated by comparing patients operated under the old and new protocols in a 1:1 propensity score match based on age, sex, and preoperative peripheral vascular resistance (PVR).
Results
Matching resulted in 56 patients (28 per group) between July 1, 2010, and May 31, 2020. The new protocol group had a lower intraoperative fluid balance (1.85 vs 6.76 liters, p < 0.001), vasoactive-inotropic score (VIS) (8.7 vs 17.7, p = 0.04), shorter operative- (407 vs 451 min, p = 0.03), and hospitalization time (LOS) (18 vs 27 days, p = 0.008). Morbidity and mortality at 30- and 90-days were similar in both groups. The new protocol was associated with reduced intraoperative fluid balance after adjustment for operative time (−3.7 liters [95% CI −5.2, −2.1], p < 0.0001). Lower intraoperative fluid balance was associated with shorter hospitalization in the intensive care unit, intubation time, LOS, and lower VIS (p = 0.0011, 0.0013, 0.008, <0.0001, respectively). The protocol change shortened LOS, independent of operative time, by 27% [95% CI, 44%, 6%], p = 0.02.
Conclusions
Priming and maintenance protocol for CPB with the addition of 5% HA had a beneficial effect on intraoperative fluid balance and improved outcome after PEA for patients with CTEPH.
背景:肺动脉内膜切除术(PEA)采用深度低温循环停止(DHCA)和体外循环(CPB)是慢性血栓栓塞性肺动脉高压(CTEPH)的首选治疗方法。晶体引液引起血液稀释,缺点是没有PEA标准。本研究评估了PEA期间在CPB-prime和血液稀释溶液中加入5%人白蛋白(HA)后CTEPH患者的预后。方法以年龄、性别、术前外周血管阻力(PVR)为指标,以1:1的倾向性评分对cpb方案变更的效果进行比较。结果在2010年7月1日至2020年5月31日期间,匹配了56例患者(每组28例)。新方案组术中液体平衡较低(1.85 vs 6.76升,p <;0.001)、血管活性-肌力评分(VIS) (8.7 vs 17.7, p = 0.04)、较短手术时间(407 vs 451 min, p = 0.03)和住院时间(LOS) (18 vs 27天,p = 0.008)。两组在30天和90天的发病率和死亡率相似。新方案与调整手术时间后术中液体平衡降低相关(- 3.7升[95% CI - 5.2, - 2.1], p <;0.0001)。较低的术中液体平衡与较短的重症监护病房住院时间、插管时间、LOS和较低的VIS相关(p分别= 0.0011、0.0013、0.008和0.0001)。方案的改变使LOS缩短了27%,与手术时间无关[95% CI, 44%, 6%], p = 0.02。结论添加5% HA的CPB启动和维持方案对CTEPH患者术中液体平衡和PEA后预后有良好影响。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


