Marc Strik, Sylvain Ploux, Anand Thiyagarajah, Lars van Krimpen, Pierre Bordachar
{"title":"Hitting the Wall: The Hidden Challenge of 2:1 Block in Pacemaker Patients.","authors":"Marc Strik, Sylvain Ploux, Anand Thiyagarajah, Lars van Krimpen, Pierre Bordachar","doi":"10.1111/pace.70006","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Dual-chamber pacemakers incorporate proprietary algorithms to optimize atrioventricular (AV) synchronization and prevent pacemaker-mediated arrhythmias. Patients have recently presented to our center with severe exercise intolerance due to the early onset of 2:1 AV block caused by Biotronik's Auto-PVARP and 2:1 Lock-in protection algorithms. This study evaluates the relationship of these algorithms to low 2:1 block rates in a large cohort of remotely monitored pacemaker patients.</p><p><strong>Methods: </strong>We troubleshooted the patients with symptomatic exercise intolerance. We then performed an observational study using remote monitoring data from 895 patients implanted with Biotronik pacemakers, programmed in DDD(R) mode with the Auto-PVARP algorithm activated. We analyzed PVARP settings, 2:1 block rates, and their relationship with age-predicted maximal sinus rates.</p><p><strong>Results: </strong>Among the 895 remotely monitored patients, the majority had significantly prolonged PVARP settings, lowering their 2:1 block rate. At the most recent transmission, only 37% had a PVARP ≤225 ms, while 63% had longer values (275-375 ms), leading to lower 2:1 block thresholds. The 2:1 block rate was below the age-predicted maximal sinus rate in 48% of patients, suggesting a high risk of pacing-induced exercise limitations. The prolonged PVARP was largely driven by Auto-PVARP extensions, often without documented pacemaker-mediated tachycardia (PMT). These findings indicate that a significant proportion of pacemaker-dependent patients may unknowingly experience pacing-related exercise intolerance.</p><p><strong>Conclusion: </strong>The Biotronik Auto-PVARP algorithm frequently extends the refractory period, lowering the threshold for 2:1 block and potentially limiting exercise capacity in active patients. Disabling Auto-PVARP and setting a fixed, shorter PVARP may improve exercise tolerance.</p>","PeriodicalId":520740,"journal":{"name":"Pacing and clinical electrophysiology : PACE","volume":" ","pages":"953-958"},"PeriodicalIF":1.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12439231/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pacing and clinical electrophysiology : PACE","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/pace.70006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
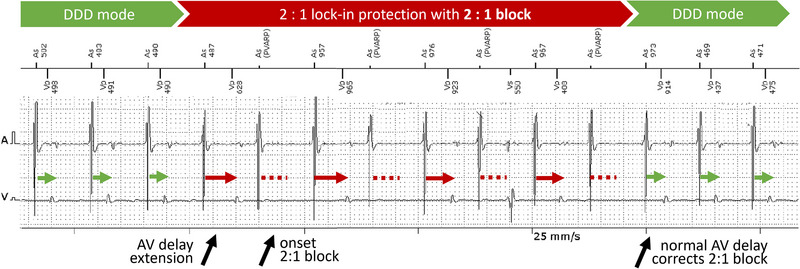
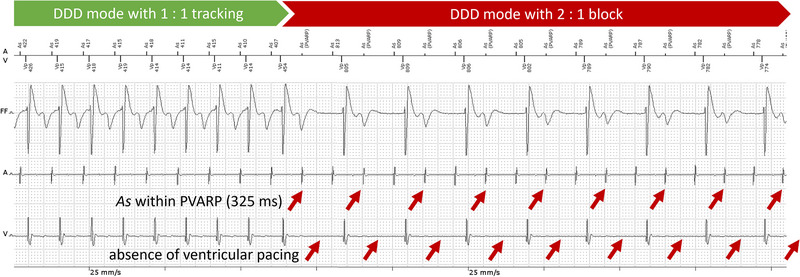
Introduction: Dual-chamber pacemakers incorporate proprietary algorithms to optimize atrioventricular (AV) synchronization and prevent pacemaker-mediated arrhythmias. Patients have recently presented to our center with severe exercise intolerance due to the early onset of 2:1 AV block caused by Biotronik's Auto-PVARP and 2:1 Lock-in protection algorithms. This study evaluates the relationship of these algorithms to low 2:1 block rates in a large cohort of remotely monitored pacemaker patients.
Methods: We troubleshooted the patients with symptomatic exercise intolerance. We then performed an observational study using remote monitoring data from 895 patients implanted with Biotronik pacemakers, programmed in DDD(R) mode with the Auto-PVARP algorithm activated. We analyzed PVARP settings, 2:1 block rates, and their relationship with age-predicted maximal sinus rates.
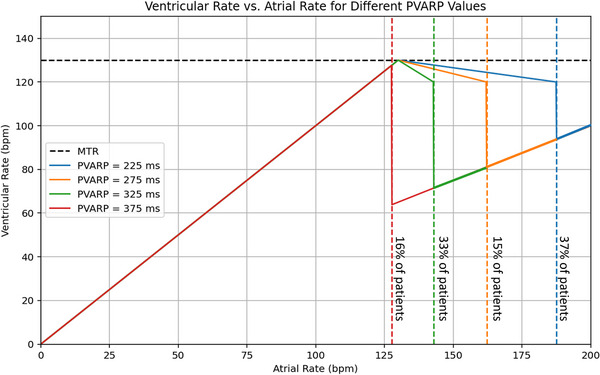
Results: Among the 895 remotely monitored patients, the majority had significantly prolonged PVARP settings, lowering their 2:1 block rate. At the most recent transmission, only 37% had a PVARP ≤225 ms, while 63% had longer values (275-375 ms), leading to lower 2:1 block thresholds. The 2:1 block rate was below the age-predicted maximal sinus rate in 48% of patients, suggesting a high risk of pacing-induced exercise limitations. The prolonged PVARP was largely driven by Auto-PVARP extensions, often without documented pacemaker-mediated tachycardia (PMT). These findings indicate that a significant proportion of pacemaker-dependent patients may unknowingly experience pacing-related exercise intolerance.
Conclusion: The Biotronik Auto-PVARP algorithm frequently extends the refractory period, lowering the threshold for 2:1 block and potentially limiting exercise capacity in active patients. Disabling Auto-PVARP and setting a fixed, shorter PVARP may improve exercise tolerance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


