{"title":"Deriving severity thresholds of treatment burden for the patient experience with treatment and self-management (PETS).","authors":"David T Eton, Kathleen J Yost","doi":"10.1177/26335565251350923","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The Patient Experience with Treatment and Self-management (PETS) is a valid self-report measure of treatment burden. The objective of this analysis is to determine severity cut points for its scores.</p><p><strong>Methods: </strong>Data from two survey studies of adults with multimorbidity were used to determine estimates of low, moderate, and high burden for twelve PETS scores. Anchor-based analyses were used to map mean PETS scores onto scores of other self-report measures, including physical and mental health, self-efficacy, and activity limitations. Low, medium, and high scores on the anchors were based on published thresholds or tertile splits of score distributions. Mean PETS scores were compared across levels of the anchor variable using analysis of variance (ANOVA) then summarized to produce burden severity cut points.</p><p><strong>Results: </strong>Study 1 featured survey data from 332 adults with multimorbidity (mean age = 66 years, 56% female); study 2 featured survey data from 439 adults with multimorbidity (mean age = 60 years, 62% female). Anchor measures were correlated with PETS scores at rho≥ 0.30. ANOVAs comparing PETS scores across the levels of each anchor variable were all significant (<i>p</i>s< .001). Estimates were placed into data tables. Cut scores for discriminating treatment burden severity levels were identified as the midpoint between the mean PETS scores associated with adjacent anchor categories (e.g., low vs. medium and medium vs. high burden), rounded to the nearest whole number.</p><p><strong>Conclusions: </strong>Severity thresholds can improve the interpretability of PETS scores. The preliminary estimates derived require verification in future studies.</p>","PeriodicalId":73843,"journal":{"name":"Journal of multimorbidity and comorbidity","volume":"15 ","pages":"26335565251350923"},"PeriodicalIF":3.0000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185958/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of multimorbidity and comorbidity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26335565251350923","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The Patient Experience with Treatment and Self-management (PETS) is a valid self-report measure of treatment burden. The objective of this analysis is to determine severity cut points for its scores.
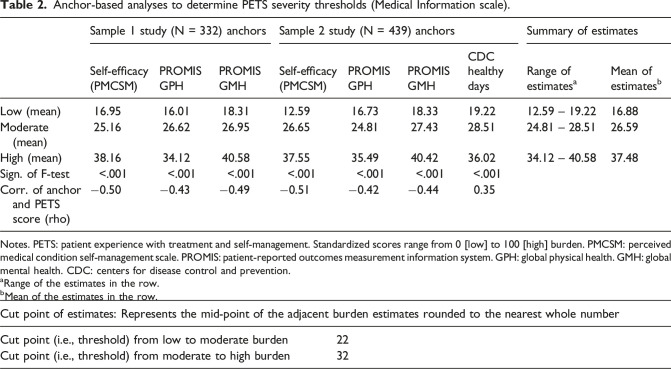
Methods: Data from two survey studies of adults with multimorbidity were used to determine estimates of low, moderate, and high burden for twelve PETS scores. Anchor-based analyses were used to map mean PETS scores onto scores of other self-report measures, including physical and mental health, self-efficacy, and activity limitations. Low, medium, and high scores on the anchors were based on published thresholds or tertile splits of score distributions. Mean PETS scores were compared across levels of the anchor variable using analysis of variance (ANOVA) then summarized to produce burden severity cut points.
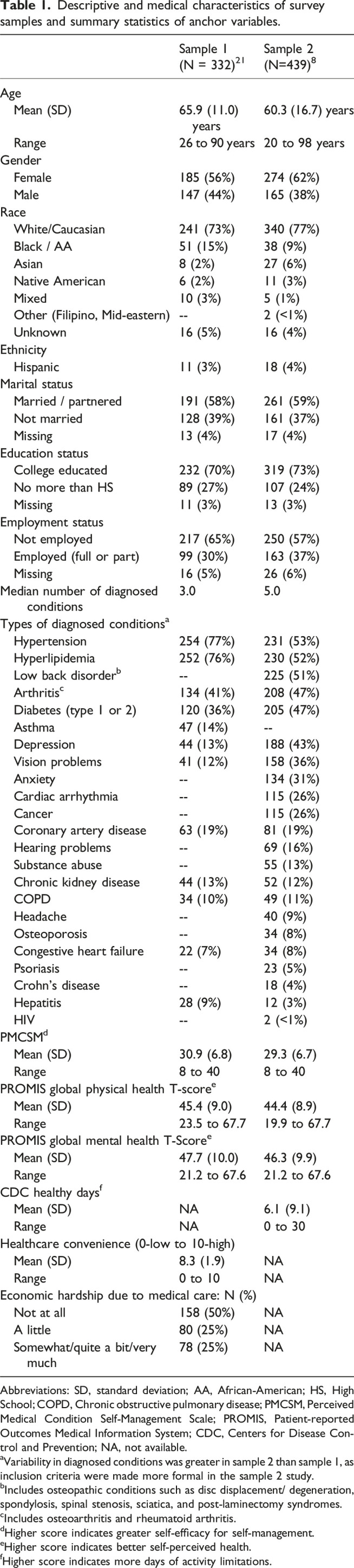
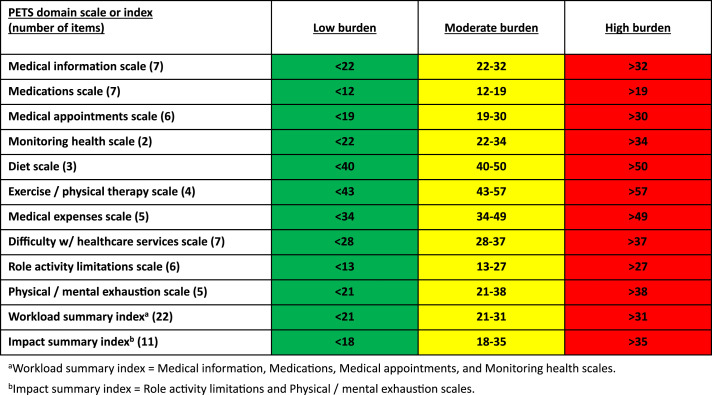
Results: Study 1 featured survey data from 332 adults with multimorbidity (mean age = 66 years, 56% female); study 2 featured survey data from 439 adults with multimorbidity (mean age = 60 years, 62% female). Anchor measures were correlated with PETS scores at rho≥ 0.30. ANOVAs comparing PETS scores across the levels of each anchor variable were all significant (ps< .001). Estimates were placed into data tables. Cut scores for discriminating treatment burden severity levels were identified as the midpoint between the mean PETS scores associated with adjacent anchor categories (e.g., low vs. medium and medium vs. high burden), rounded to the nearest whole number.
Conclusions: Severity thresholds can improve the interpretability of PETS scores. The preliminary estimates derived require verification in future studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


