Song Peng Ang, Eunseuk Lee, Jia Ee Chia, Maya Iglesias, Mariela Di Vanna, Shreya Shambhavi, Jose Iglesias
{"title":"Time-to-Treatment Initiation and Its Effect on All-Cause Mortality: Insights From the Surveillance, Epidemiology, and End Results Database.","authors":"Song Peng Ang, Eunseuk Lee, Jia Ee Chia, Maya Iglesias, Mariela Di Vanna, Shreya Shambhavi, Jose Iglesias","doi":"10.14740/wjon2584","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Delays in cancer treatment initiation can significantly impact survival outcomes, but the magnitude of this effect varies by cancer type, stage, and patient demographics. This study examined the association between time-to-treatment initiation (TTI) and all-cause mortality across multiple common cancers, evaluating differential impacts and sociodemographic disparities.</p><p><strong>Methods: </strong>A retrospective cohort analysis was conducted using the Surveillance, Epidemiology, and End Results (SEER) database, including 991,771 adults diagnosed with breast, lung, prostate, or colorectal cancers between 2015 and 2020. TTI intervals were divided into four categories: 0 - 1, 2 - 5, 6 - 9, and ≥ 10 months. Cox proportional hazards models, adjusted for demographic, socioeconomic, cancer-specific, and treatment factors, assessed the impact of TTI on all-cause mortality, accounting for time-varying covariates.</p><p><strong>Results: </strong>Overall, 63.9% of patients initiated treatment within 1 month. Unadjusted analyses revealed paradoxically lower mortality with longer TTI intervals (26.1% for 0 - 1 month vs. 11.4% for ≥ 10 months). After adjusting for time-varying effects, longer TTI significantly correlated with higher mortality risks (hazard ratio (HR): 1.02 for 2 - 5 months, 1.08 for 6 - 9 months, 1.23 for ≥ 10 months; P < 0.001 each), compared to treatment within 1 month. Older age (HR: 1.06), male gender (HR: 1.08), unmarried status (HR: 1.06), and non-Hispanic Black race (HR: 1.03) were independently associated with increased mortality. Lung cancer patients had significantly higher mortality than breast, prostate, and colorectal cancers (all P < 0.001). Treatment differences emerged, with reduced chemotherapy (40.2% to 10.0%) and surgical interventions (70.6% to 48.8%) at longer intervals.</p><p><strong>Conclusion: </strong>Our analysis showed that increased TTI is independently associated with significantly higher all-cause mortality across major cancers, emphasizing the urgency of timely treatment initiation. Sociodemographic disparities in TTI and outcomes highlight systemic barriers disproportionately affecting vulnerable populations, necessitating targeted interventions to improve equitable cancer care and survival outcomes.</p>","PeriodicalId":46797,"journal":{"name":"World Journal of Oncology","volume":"16 3","pages":"286-294"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185122/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/wjon2584","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Delays in cancer treatment initiation can significantly impact survival outcomes, but the magnitude of this effect varies by cancer type, stage, and patient demographics. This study examined the association between time-to-treatment initiation (TTI) and all-cause mortality across multiple common cancers, evaluating differential impacts and sociodemographic disparities.
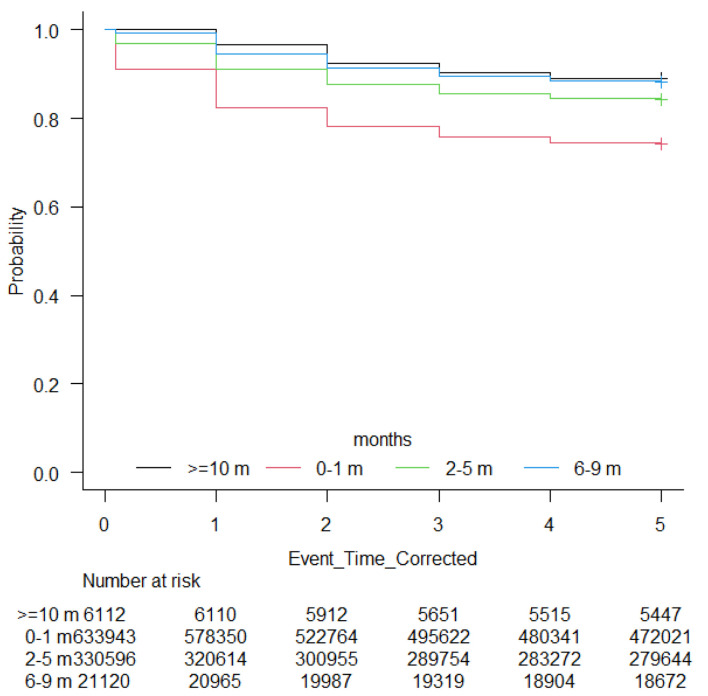
Methods: A retrospective cohort analysis was conducted using the Surveillance, Epidemiology, and End Results (SEER) database, including 991,771 adults diagnosed with breast, lung, prostate, or colorectal cancers between 2015 and 2020. TTI intervals were divided into four categories: 0 - 1, 2 - 5, 6 - 9, and ≥ 10 months. Cox proportional hazards models, adjusted for demographic, socioeconomic, cancer-specific, and treatment factors, assessed the impact of TTI on all-cause mortality, accounting for time-varying covariates.
Results: Overall, 63.9% of patients initiated treatment within 1 month. Unadjusted analyses revealed paradoxically lower mortality with longer TTI intervals (26.1% for 0 - 1 month vs. 11.4% for ≥ 10 months). After adjusting for time-varying effects, longer TTI significantly correlated with higher mortality risks (hazard ratio (HR): 1.02 for 2 - 5 months, 1.08 for 6 - 9 months, 1.23 for ≥ 10 months; P < 0.001 each), compared to treatment within 1 month. Older age (HR: 1.06), male gender (HR: 1.08), unmarried status (HR: 1.06), and non-Hispanic Black race (HR: 1.03) were independently associated with increased mortality. Lung cancer patients had significantly higher mortality than breast, prostate, and colorectal cancers (all P < 0.001). Treatment differences emerged, with reduced chemotherapy (40.2% to 10.0%) and surgical interventions (70.6% to 48.8%) at longer intervals.
Conclusion: Our analysis showed that increased TTI is independently associated with significantly higher all-cause mortality across major cancers, emphasizing the urgency of timely treatment initiation. Sociodemographic disparities in TTI and outcomes highlight systemic barriers disproportionately affecting vulnerable populations, necessitating targeted interventions to improve equitable cancer care and survival outcomes.
期刊介绍:
World Journal of Oncology, bimonthly, publishes original contributions describing basic research and clinical investigation of cancer, on the cellular, molecular, prevention, diagnosis, therapy and prognosis aspects. The submissions can be basic research or clinical investigation oriented. This journal welcomes those submissions focused on the clinical trials of new treatment modalities for cancer, and those submissions focused on molecular or cellular research of the oncology pathogenesis. Case reports submitted for consideration of publication should explore either a novel genomic event/description or a new safety signal from an oncolytic agent. The areas of interested manuscripts are these disciplines: tumor immunology and immunotherapy; cancer molecular pharmacology and chemotherapy; drug sensitivity and resistance; cancer epidemiology; clinical trials; cancer pathology; radiobiology and radiation oncology; solid tumor oncology; hematological malignancies; surgical oncology; pediatric oncology; molecular oncology and cancer genes; gene therapy; cancer endocrinology; cancer metastasis; prevention and diagnosis of cancer; other cancer related subjects. The types of manuscripts accepted are original article, review, editorial, short communication, case report, letter to the editor, book review.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


