Evaluating the Impact of Community-Based Medical Education on Health Literacy and Patient Empowerment in Underserved Populations: A Pilot Cohort Study.
Aida Aljafri, Persia Abba, Anita Sedghi, Andreas Conte, Waseem Jerjes
{"title":"Evaluating the Impact of Community-Based Medical Education on Health Literacy and Patient Empowerment in Underserved Populations: A Pilot Cohort Study.","authors":"Aida Aljafri, Persia Abba, Anita Sedghi, Andreas Conte, Waseem Jerjes","doi":"10.3390/clinpract15060097","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Traditionally, community-based education (CBE) programmes have been utilised for teaching medical students clinical and interpersonal skills through placement in underserved environments. This pilot cohort study tested an extended model of CBE by infusing patient education into student-conducted consultations with the dual objectives of stimulating improved learning for the students and improved health literacy for the patients. <b>Methods:</b> The intervention involved 38 final-year medical students and 85 adult patients and from underprivileged communities in North West London. The students first undertook online preparatory workshops on health literacy, communication skills, and cultural competence. Subsequently, they imparted 20-30 min educational sessions on chronic disease management and preventive care to the patients on their clinical placements. The quantitative measurement used pre- and post-intervention questionnaires, and the qualitative measurement was based on reflective diaries and patient feedback. Paired <i>t</i>-tests were used for statistical comparisons, while a thematic analysis was used for textual answers. <b>Results:</b> Student confidence in breaking down medical jargon improved from 2.8 ± 0.7 to 4.4 ± 0.5 (<i>p</i> < 0.01), and confidence in making use of visual aids improved from 2.5 ± 0.8 to 4.2 ± 0.6 (<i>p</i> < 0.01). Understanding among the patients of their health conditions improved from 27% to 74% (<i>p</i> < 0.001), and self-confidence in their ability to manage their health improved from 31% to 79% (<i>p</i> < 0.001). The qualitative feedback noted improved empathy, cultural sensitivity, and a positive effect on patient empowerment through tailored education. <b>Conclusions:</b> This CBE intervention had two benefits: improving teaching and communication skills in students and greatly enhancing health literacy in underserved patients. The integration of structured education into usual care encounters holds the promise of a scalable, sustainable method for addressing health disparities. Longer longitudinal studies are necessary to assess its long-term success and incorporation into medical education.</p>","PeriodicalId":45306,"journal":{"name":"Clinics and Practice","volume":"15 6","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12191660/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/clinpract15060097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
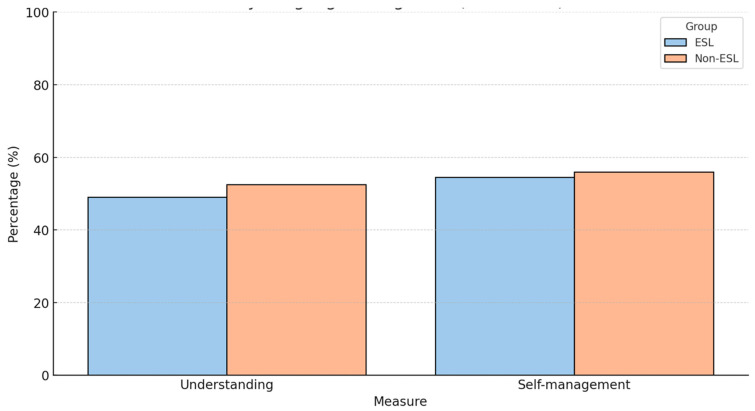
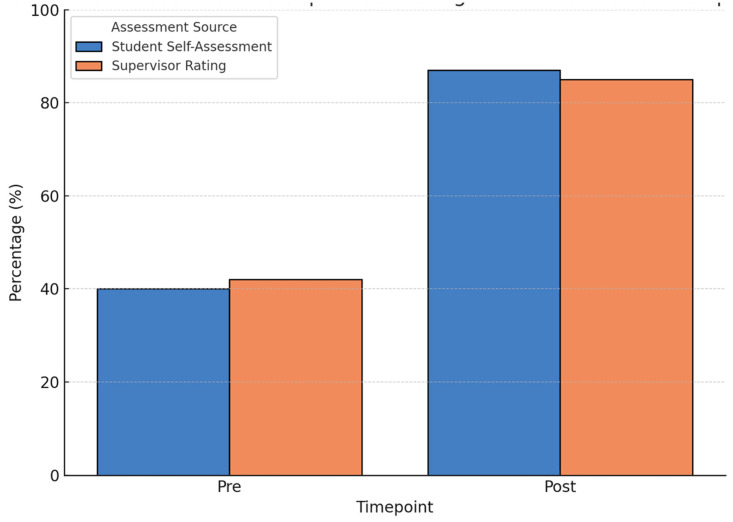
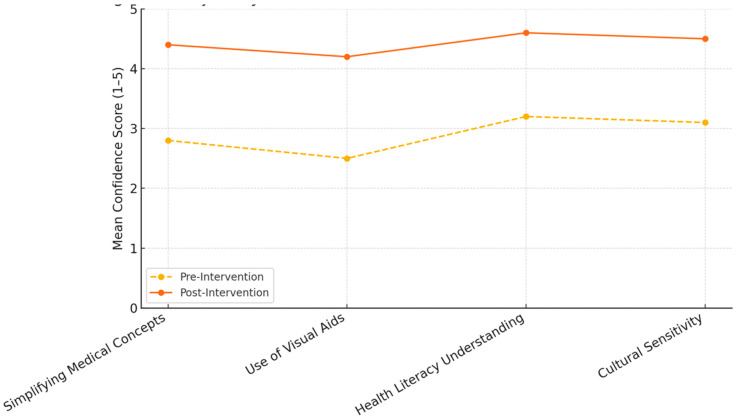
Background: Traditionally, community-based education (CBE) programmes have been utilised for teaching medical students clinical and interpersonal skills through placement in underserved environments. This pilot cohort study tested an extended model of CBE by infusing patient education into student-conducted consultations with the dual objectives of stimulating improved learning for the students and improved health literacy for the patients. Methods: The intervention involved 38 final-year medical students and 85 adult patients and from underprivileged communities in North West London. The students first undertook online preparatory workshops on health literacy, communication skills, and cultural competence. Subsequently, they imparted 20-30 min educational sessions on chronic disease management and preventive care to the patients on their clinical placements. The quantitative measurement used pre- and post-intervention questionnaires, and the qualitative measurement was based on reflective diaries and patient feedback. Paired t-tests were used for statistical comparisons, while a thematic analysis was used for textual answers. Results: Student confidence in breaking down medical jargon improved from 2.8 ± 0.7 to 4.4 ± 0.5 (p < 0.01), and confidence in making use of visual aids improved from 2.5 ± 0.8 to 4.2 ± 0.6 (p < 0.01). Understanding among the patients of their health conditions improved from 27% to 74% (p < 0.001), and self-confidence in their ability to manage their health improved from 31% to 79% (p < 0.001). The qualitative feedback noted improved empathy, cultural sensitivity, and a positive effect on patient empowerment through tailored education. Conclusions: This CBE intervention had two benefits: improving teaching and communication skills in students and greatly enhancing health literacy in underserved patients. The integration of structured education into usual care encounters holds the promise of a scalable, sustainable method for addressing health disparities. Longer longitudinal studies are necessary to assess its long-term success and incorporation into medical education.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


