Joseph M Unger, Hillary S Andrews, Laura A Levit, Brittany A McKelvey, Mark Stewart, Beverly Canin, Keith Flaherty, Denise Kimball, Therica Miller, Adedayo Onitilo, Suanna Bruinooge, Elizabeth Garrett-Mayer, Caroline Schenkel
{"title":"Impact of the COVID-19 Pandemic Mitigation Strategies on Cancer Treatment Trials: A Meta-Analysis of Industry and National Cancer Institute Studies.","authors":"Joseph M Unger, Hillary S Andrews, Laura A Levit, Brittany A McKelvey, Mark Stewart, Beverly Canin, Keith Flaherty, Denise Kimball, Therica Miller, Adedayo Onitilo, Suanna Bruinooge, Elizabeth Garrett-Mayer, Caroline Schenkel","doi":"10.1200/OA-25-00021","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The onset of the COVID-19 pandemic in early 2020 disrupted the conduct of cancer clinical trials. In response, federal agencies allowed more flexibility for trial recruitment and patient follow-up. A key question is whether the benefits of adopting these strategies outweigh the potential detriments to quality metrics.</p><p><strong>Methods: </strong>A joint ASCO and Friends of Cancer Research task force invited industry and National Cancer Institute trial sponsors to contribute deidentified trial-level aggregate data on enrollment, major protocol deviations, dropouts, and severe adverse events (Common Terminology Criteria for Adverse Events grade 3-5). These quality metrics were examined as proportions of participants at risk during the pre-COVID-19 (January 2017-February, 2020), initial wave (March-April, 2020), initial recovery (May-December, 2020), and secondary recovery (January 2021-December 2022) periods. Multilevel beta-regression was used, adjusting for phase; study and sponsor were treated as random effects. Indicator variables were used with pre-COVID-19 as the reference.</p><p><strong>Results: </strong>Ten sponsors contributed 67 analyzable trials with N = 12,000 US-based participants. Enrollment odds decreased 49% in the initial wave (odds ratio [OR], 0.51 [95% CI, 0.30 to 0.86], <i>P</i> = .01) but recovered to pre-COVID-19 levels by 2021-2022 (OR, 1.01 [95% CI, 0.56 to 1.81], <i>P</i> = .97). Major protocol deviations, dropouts, and severe toxicity all had a lower incidence in the initial wave compared with pre-COVID-19; these outcomes were also less frequent (<i>P</i> < .05) in the initial recovery period but returned to pre-COVID-19 levels by 2021-2022.</p><p><strong>Conclusion: </strong>In this multicollaborator evaluation, large declines in enrollment, major protocol deviations, dropouts, and severe toxicity during the acute phase of the pandemic all returned to pre-COVID-19 levels by 2021-2022. These findings highlight the impact of the temporary disruption to trial conduct during the pandemic's peak, but suggest that pandemic-related procedural flexibility did not result in long-term reduced data quality. Sponsors and regulators should consider broader adaptation of trial flexibilities moving forward.</p>","PeriodicalId":520350,"journal":{"name":"JCO oncology advances","volume":"2 1","pages":"e2500021"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178165/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCO oncology advances","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1200/OA-25-00021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The onset of the COVID-19 pandemic in early 2020 disrupted the conduct of cancer clinical trials. In response, federal agencies allowed more flexibility for trial recruitment and patient follow-up. A key question is whether the benefits of adopting these strategies outweigh the potential detriments to quality metrics.
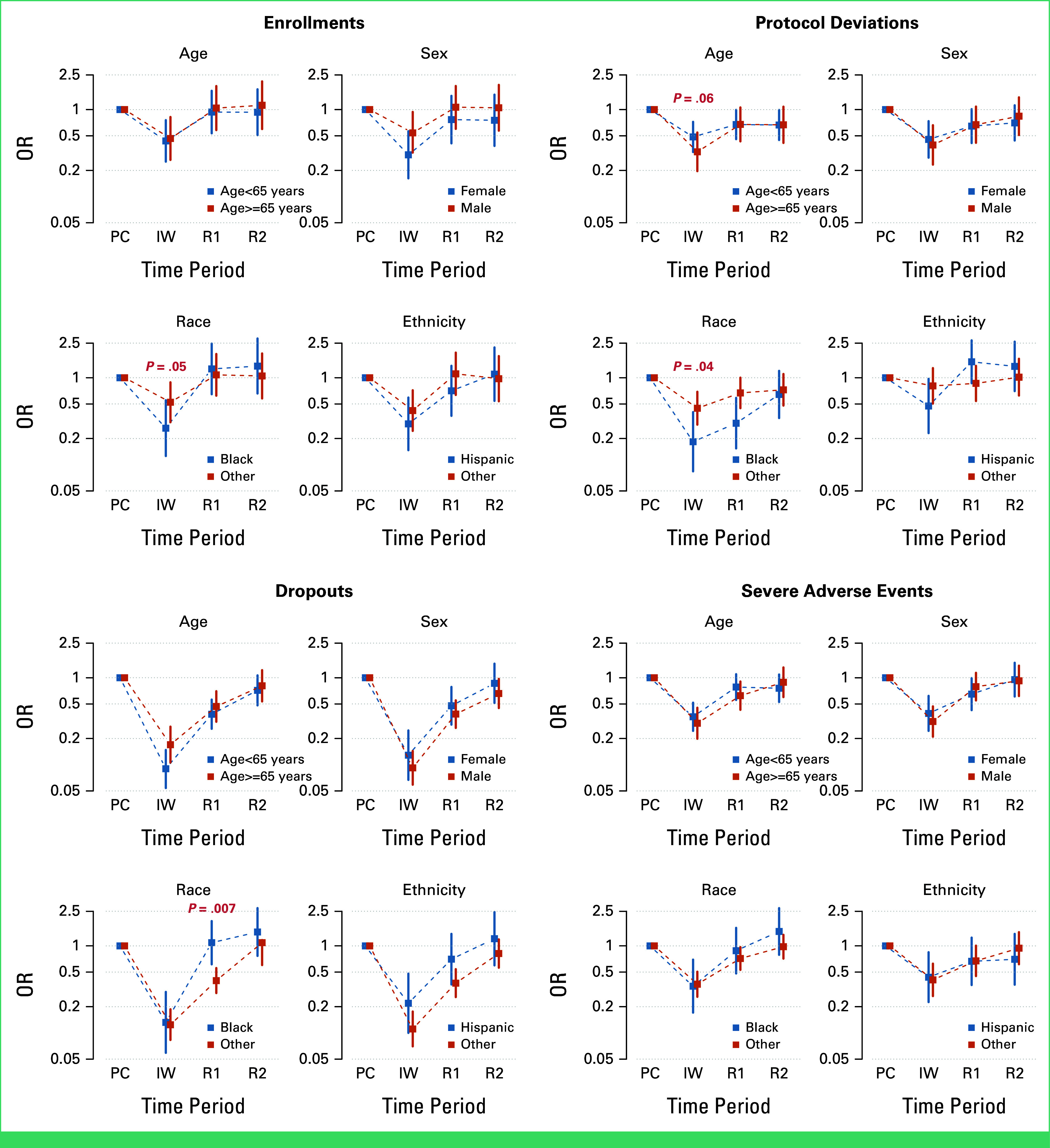
Methods: A joint ASCO and Friends of Cancer Research task force invited industry and National Cancer Institute trial sponsors to contribute deidentified trial-level aggregate data on enrollment, major protocol deviations, dropouts, and severe adverse events (Common Terminology Criteria for Adverse Events grade 3-5). These quality metrics were examined as proportions of participants at risk during the pre-COVID-19 (January 2017-February, 2020), initial wave (March-April, 2020), initial recovery (May-December, 2020), and secondary recovery (January 2021-December 2022) periods. Multilevel beta-regression was used, adjusting for phase; study and sponsor were treated as random effects. Indicator variables were used with pre-COVID-19 as the reference.
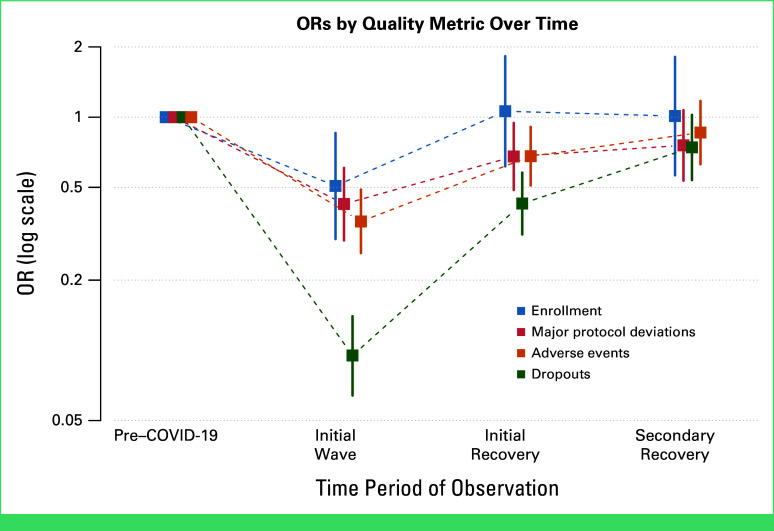
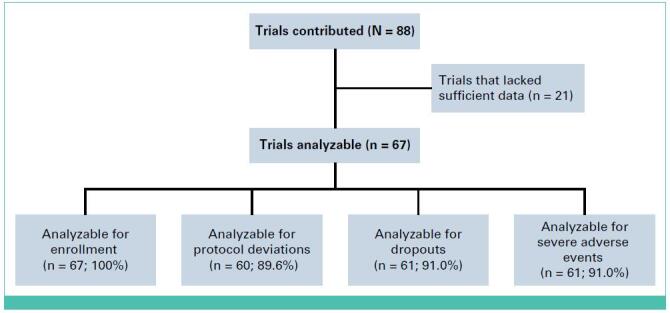
Results: Ten sponsors contributed 67 analyzable trials with N = 12,000 US-based participants. Enrollment odds decreased 49% in the initial wave (odds ratio [OR], 0.51 [95% CI, 0.30 to 0.86], P = .01) but recovered to pre-COVID-19 levels by 2021-2022 (OR, 1.01 [95% CI, 0.56 to 1.81], P = .97). Major protocol deviations, dropouts, and severe toxicity all had a lower incidence in the initial wave compared with pre-COVID-19; these outcomes were also less frequent (P < .05) in the initial recovery period but returned to pre-COVID-19 levels by 2021-2022.
Conclusion: In this multicollaborator evaluation, large declines in enrollment, major protocol deviations, dropouts, and severe toxicity during the acute phase of the pandemic all returned to pre-COVID-19 levels by 2021-2022. These findings highlight the impact of the temporary disruption to trial conduct during the pandemic's peak, but suggest that pandemic-related procedural flexibility did not result in long-term reduced data quality. Sponsors and regulators should consider broader adaptation of trial flexibilities moving forward.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


