Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North).
Tricia S Williams, Angela Deotto, Andrea Greenblatt, Giulia F Fabiano, Rivka Green, Janaksha Linga-Easwaran, Evdokia Anagnostou, Jennifer Crosbie, Elizabeth Kelley, Steven P Miller, Rob Nicolson, Jennifer Rosart, Shari L Wade, Melanie Barwick
{"title":"Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North).","authors":"Tricia S Williams, Angela Deotto, Andrea Greenblatt, Giulia F Fabiano, Rivka Green, Janaksha Linga-Easwaran, Evdokia Anagnostou, Jennifer Crosbie, Elizabeth Kelley, Steven P Miller, Rob Nicolson, Jennifer Rosart, Shari L Wade, Melanie Barwick","doi":"10.1177/26334895251346816","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clinicians, health care organizations, and families demand better and more accessible children's mental health services with greater patient engagement. The I-InTERACT-North program was developed for children following traumatic brain injury and adapted for a transdiagnostic neurological and neurodevelopmental focus, with a recent transition to a stepped-care model. To date, the program has been exclusively provided within research studies; however, demand for its clinical use is growing. Implementation frameworks provide essential guidance regarding facilitators and barriers of clinical implementation under real-world conditions. Similarly, intersectionality evaluation can provide insights to develop equitable and inclusive health care practices. Informed by the Consolidated Framework of Implementation Research 2.0 (CFIR) and recent intersectionality supplement, the objectives were to examine the perspectives of parents/caregivers and clinical partners involved in the I-InTERACT-North program to identify (a) facilitators and barriers to inform the scale and spread of the program, and (b) equity, diversity, and inclusion (EDI) considerations to integrate in future clinical implementation.</p><p><strong>Method: </strong>This study used a qualitative descriptive design with focus group methodology. Participants included parents/caregivers and clinical partners. Semi-structured focus groups were conducted virtually. Focus group data were coded inductively and deductively using CFIR 2.0. The team reflected on intersectionality in the data, coding results, and broader context of the program's history.</p><p><strong>Results: </strong>Positive perceptions of the innovation's relevance and adaptability were echoed across focus groups. Prominent facilitators included the program's adaptability, personalized, flexible format, and knowledge dissemination. Barriers included geography, technological accessibility, and workflow, with participants stressing the importance of tailoring to culture, language, and neurodiversity. Feedback from participants aligned with 10 reflective prompts highlighted within the CFIR intersectionality supplement pertaining to families' intersecting categories, diverse intervention experiences, and information access.</p><p><strong>Conclusions: </strong>Identified facilitators of I-InTERACT-North implementation extended across program knowledge sharing and recruitment. Recommendations included directions for clinical and system integration to facilitate scalability.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"6 ","pages":"26334895251346816"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179477/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895251346816","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Clinicians, health care organizations, and families demand better and more accessible children's mental health services with greater patient engagement. The I-InTERACT-North program was developed for children following traumatic brain injury and adapted for a transdiagnostic neurological and neurodevelopmental focus, with a recent transition to a stepped-care model. To date, the program has been exclusively provided within research studies; however, demand for its clinical use is growing. Implementation frameworks provide essential guidance regarding facilitators and barriers of clinical implementation under real-world conditions. Similarly, intersectionality evaluation can provide insights to develop equitable and inclusive health care practices. Informed by the Consolidated Framework of Implementation Research 2.0 (CFIR) and recent intersectionality supplement, the objectives were to examine the perspectives of parents/caregivers and clinical partners involved in the I-InTERACT-North program to identify (a) facilitators and barriers to inform the scale and spread of the program, and (b) equity, diversity, and inclusion (EDI) considerations to integrate in future clinical implementation.
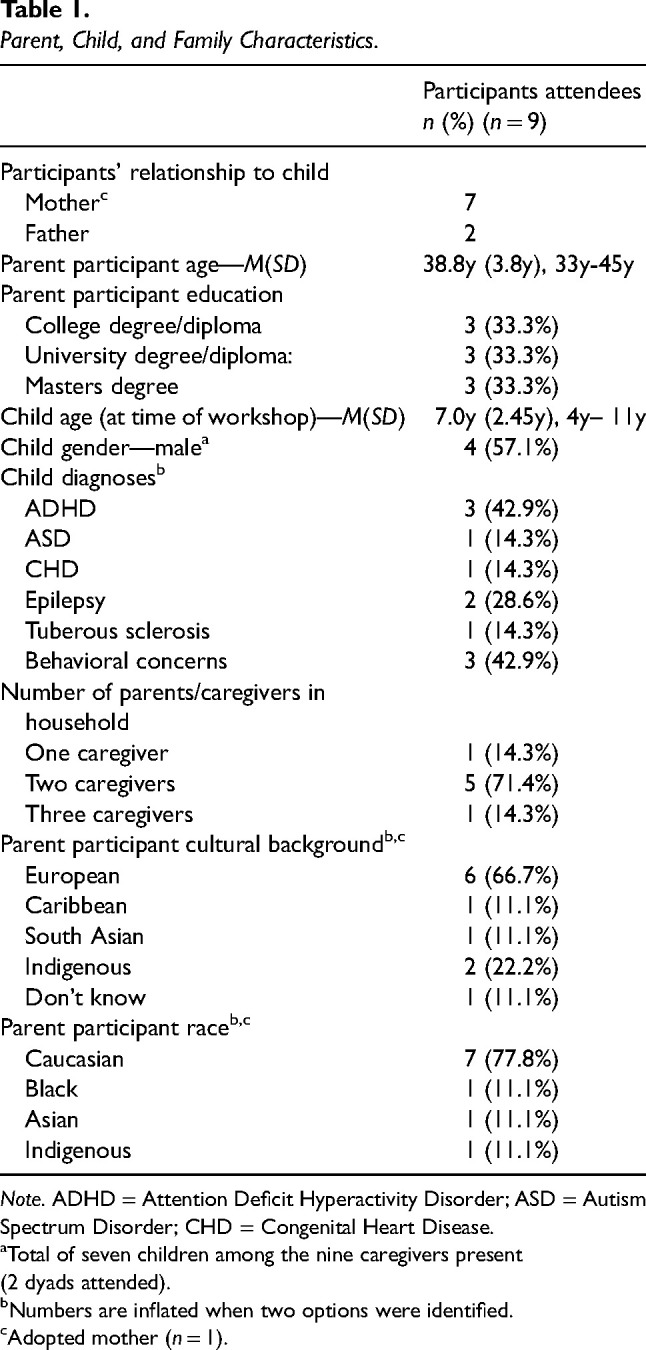
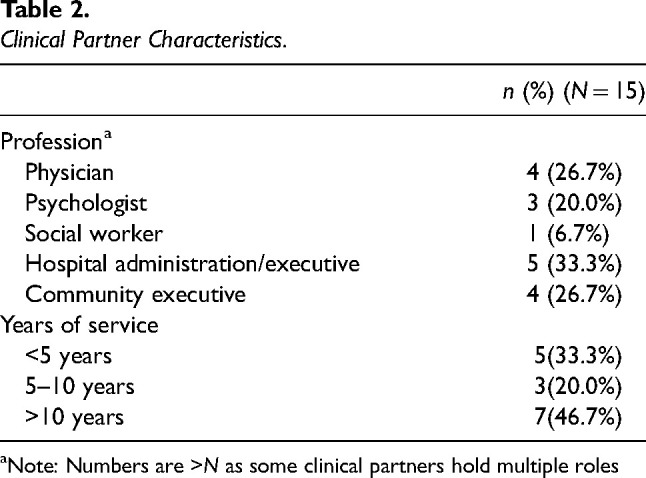
Method: This study used a qualitative descriptive design with focus group methodology. Participants included parents/caregivers and clinical partners. Semi-structured focus groups were conducted virtually. Focus group data were coded inductively and deductively using CFIR 2.0. The team reflected on intersectionality in the data, coding results, and broader context of the program's history.
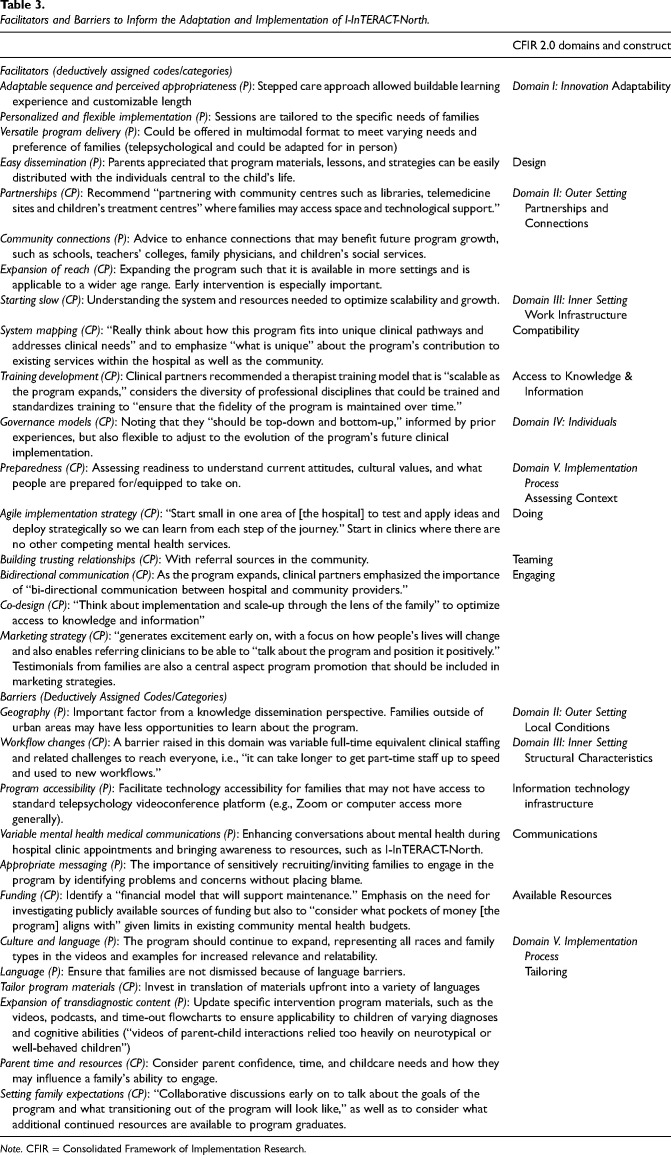
Results: Positive perceptions of the innovation's relevance and adaptability were echoed across focus groups. Prominent facilitators included the program's adaptability, personalized, flexible format, and knowledge dissemination. Barriers included geography, technological accessibility, and workflow, with participants stressing the importance of tailoring to culture, language, and neurodiversity. Feedback from participants aligned with 10 reflective prompts highlighted within the CFIR intersectionality supplement pertaining to families' intersecting categories, diverse intervention experiences, and information access.
Conclusions: Identified facilitators of I-InTERACT-North implementation extended across program knowledge sharing and recruitment. Recommendations included directions for clinical and system integration to facilitate scalability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


