Stephen Ashford, Jorge Jacinto, Klemens Fheodoroff, Lynne Turner-Stokes
{"title":"Meta-Analysis of Goal Setting and Physical Treatment Categorisation for Focal Spasticity Following Stroke or Other Acquired Brain Injury.","authors":"Stephen Ashford, Jorge Jacinto, Klemens Fheodoroff, Lynne Turner-Stokes","doi":"10.1177/27536351251343520","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Setting goals and planning treatment to attain those goals is often integral to rehabilitation practice, particularly when managing spasticity following stroke or other brain injury. Optimal treatment planning and provision using an algorithm based on mapping goals and treatments, may improve outcome.</p><p><strong>Methods: </strong>We analysed goal setting and treatment interventions through secondary analysis of goals and related treatments from (a) the Leg Activity measure study, (b) Ankle Contracture data set and (c) the Upper Limb International Spasticity-III study. Total 1207 participants. Goal categories were defined and identified based on a previously published framework: Pain, Involuntary Movement, Contracture Prevention, Active Function (self-performance of tasks), passive function (secondary performance of tasks or personal care). Treatment intervention was then identified per goal category.</p><p><strong>Results: </strong><i>Arm spasticity goal categorisation</i>: Pain 302 (22%), Involuntary Movement 166 (12%), Contracture Prevention 208 (15%), Active Function 174 (13%), passive function 501 (37%). <i>Primary interventions identified per category</i>: Pain (Positioning the limb, serial casting), Involuntary Movement (Position the limb, Splinting), Contracture Prevention (Positioning the limb, serial casting, Shoulder support and slings, Splinting), Active Function (Positioning the limb, serial casting, shoulder supports and splinting), passive function (Positioning the limb, serial casting, shoulder supports and splinting). <i>Leg spasticity goal categorisation</i>: Pain 117 (15%), Involuntary Movement 10 (1%), Contracture Prevention 139 (17%), Active Function 356 (44%), passive function 181 (22%). <i>Primary interventions identified per category</i>: Pain (Passive stretch, positioning), Involuntary Movement (Splinting), Contracture Prevention (Positioning, Orthotics, Task Practice), Active Function (Task Practice, Orthotics), passive function (Orthotics, Positioning).</p><p><strong>Conclusions: </strong>Commonalities in goal categorisation were found in arm and leg. In these cohorts' task-practice interventions to improve active function (walking and transferring) were reported for leg but were not frequently reported for arm rehabilitation. It is suggested that improved treatment planning may result in greater and faster treatment goal attainment and better outcomes.</p>","PeriodicalId":72107,"journal":{"name":"Advances in rehabilitation science and practice","volume":"14 ","pages":"27536351251343520"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179447/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in rehabilitation science and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/27536351251343520","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"0","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Setting goals and planning treatment to attain those goals is often integral to rehabilitation practice, particularly when managing spasticity following stroke or other brain injury. Optimal treatment planning and provision using an algorithm based on mapping goals and treatments, may improve outcome.
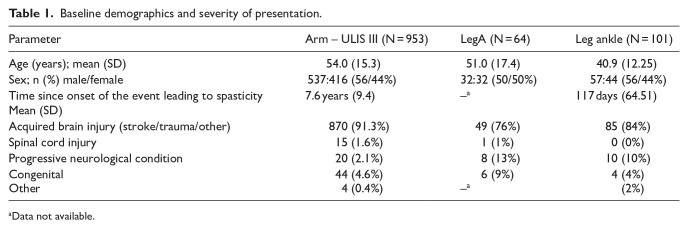
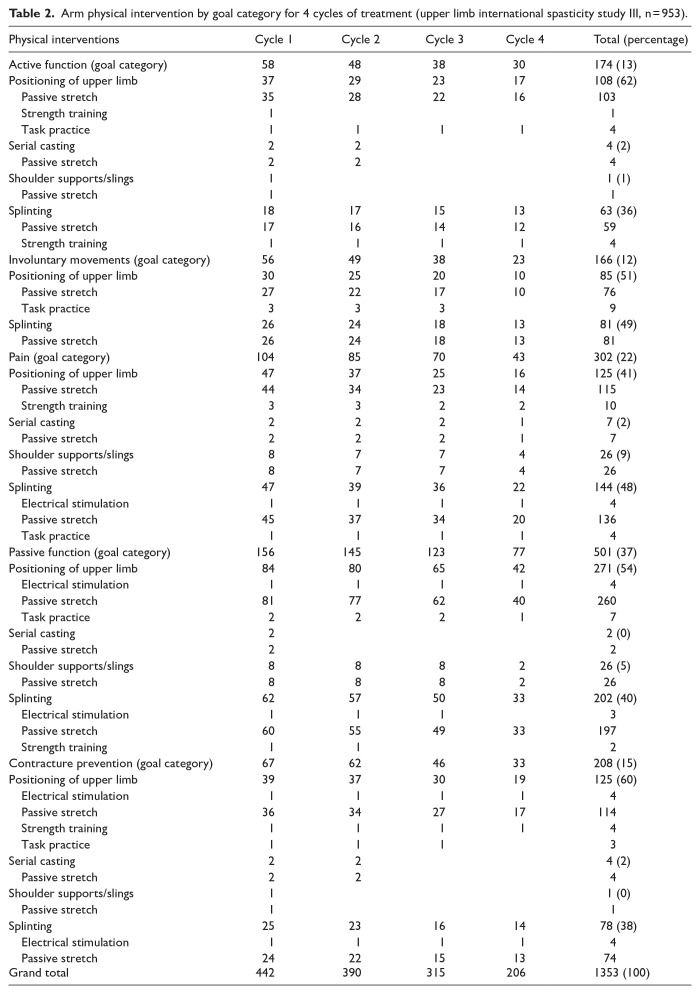
Methods: We analysed goal setting and treatment interventions through secondary analysis of goals and related treatments from (a) the Leg Activity measure study, (b) Ankle Contracture data set and (c) the Upper Limb International Spasticity-III study. Total 1207 participants. Goal categories were defined and identified based on a previously published framework: Pain, Involuntary Movement, Contracture Prevention, Active Function (self-performance of tasks), passive function (secondary performance of tasks or personal care). Treatment intervention was then identified per goal category.
Results: Arm spasticity goal categorisation: Pain 302 (22%), Involuntary Movement 166 (12%), Contracture Prevention 208 (15%), Active Function 174 (13%), passive function 501 (37%). Primary interventions identified per category: Pain (Positioning the limb, serial casting), Involuntary Movement (Position the limb, Splinting), Contracture Prevention (Positioning the limb, serial casting, Shoulder support and slings, Splinting), Active Function (Positioning the limb, serial casting, shoulder supports and splinting), passive function (Positioning the limb, serial casting, shoulder supports and splinting). Leg spasticity goal categorisation: Pain 117 (15%), Involuntary Movement 10 (1%), Contracture Prevention 139 (17%), Active Function 356 (44%), passive function 181 (22%). Primary interventions identified per category: Pain (Passive stretch, positioning), Involuntary Movement (Splinting), Contracture Prevention (Positioning, Orthotics, Task Practice), Active Function (Task Practice, Orthotics), passive function (Orthotics, Positioning).
Conclusions: Commonalities in goal categorisation were found in arm and leg. In these cohorts' task-practice interventions to improve active function (walking and transferring) were reported for leg but were not frequently reported for arm rehabilitation. It is suggested that improved treatment planning may result in greater and faster treatment goal attainment and better outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


