{"title":"Surgical Intervention for Isolated Tricuspid Valve Endocarditis-Refining Patients' Selection.","authors":"Ali Hage, Rami Abazid, Fadi Hage, Shevan Bladia, Linrui Guo, Nikolaos Tzemos","doi":"10.1055/s-0045-1808059","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we analyzed various clinical and imaging factors of patients with isolated tricuspid valve infective endocarditis (TVIE) who have undergone surgical intervention, and assessed short- and long-term outcomes after surgery.</p><p><strong>Methods: </strong>We retrospectively enrolled 26 patients diagnosed with definite isolated TVIE and underwent surgical intervention between February 2004 and August 2019. We collected patients' demographics, preoperative and postoperative data. The primary outcomes were death and a composite of the following: death, readmission with right-sided heart failure, or recurrent endocarditis.</p><p><strong>Results: </strong>A total of 29 isolated tricuspid valve surgical interventions were performed on 26 patients. The mean age was 38.6 ± 12.3 years. In total, 22/29 (75.8%) of TVIE were related to <i>Staphylococcus aureus</i> and 4/29 (13.8%) were secondary to fungal infection. During a follow-up of 5.4 ± 3.7 years, there were 9 (34.6%) deaths and 15 (57.7%) composite outcomes. Multivariable Cox regression analysis showed that male sex (hazard ratio [HR]: 16.68, 95% confidence interval [CI]: 1.63-170.34, <i>p</i> = 0.018) and intravenous drug users (IVDU) (HR: 25.66, 95% CI: 1.87-352.79, <i>p</i> = 0.015) are significantly associated with increase death; on the other hand, higher level of preoperative hemoglobin and preoperative left ventricular ejection fraction (LVEF) was found to have decreased hazard of death: HR: 0.90, 95% CI: 0.82-0.99, <i>p</i> = 0.033 and HR: 0.92, 95% CI: 0.86-0.98, <i>p</i> = 0.013, respectively.</p><p><strong>Conclusion: </strong>In our institution, surgical intervention for isolated TVIE has a mortality rate of 34.6%. Men, a history of IVDU, lower preoperative hemoglobin levels, and reduced LVEF were significant predictors of postsurgical mortality. Earlier surgical intervention for TVIE before the development of anemia or impaired LV systolic function may have a potential survival benefit.</p>","PeriodicalId":32889,"journal":{"name":"Avicenna Journal of Medicine","volume":"15 2","pages":"74-79"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178669/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Avicenna Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1808059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In this study, we analyzed various clinical and imaging factors of patients with isolated tricuspid valve infective endocarditis (TVIE) who have undergone surgical intervention, and assessed short- and long-term outcomes after surgery.
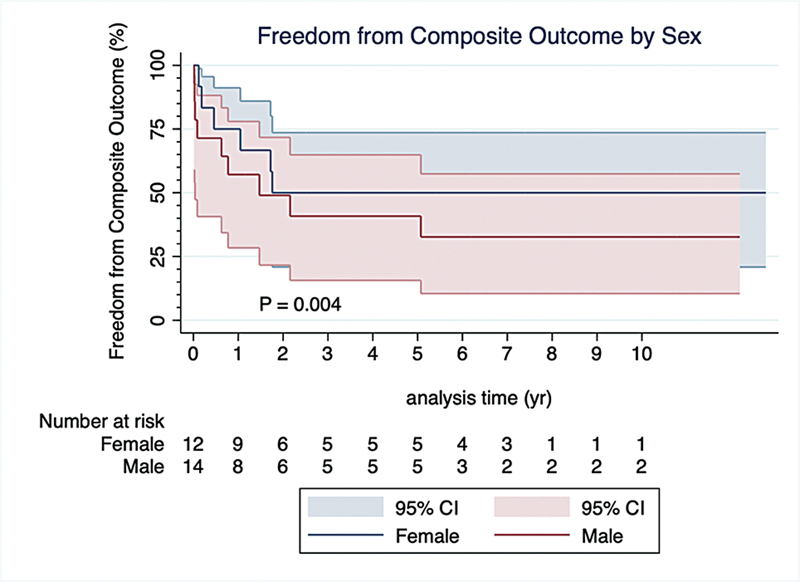
Methods: We retrospectively enrolled 26 patients diagnosed with definite isolated TVIE and underwent surgical intervention between February 2004 and August 2019. We collected patients' demographics, preoperative and postoperative data. The primary outcomes were death and a composite of the following: death, readmission with right-sided heart failure, or recurrent endocarditis.
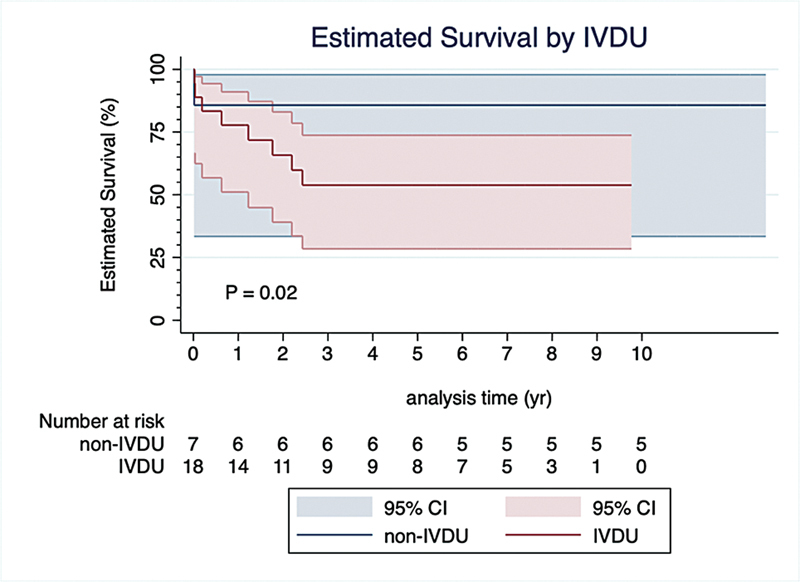
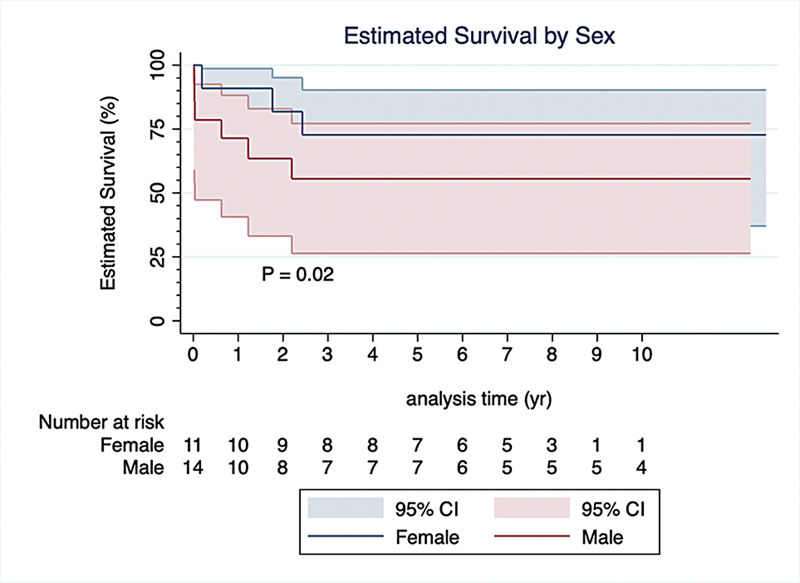
Results: A total of 29 isolated tricuspid valve surgical interventions were performed on 26 patients. The mean age was 38.6 ± 12.3 years. In total, 22/29 (75.8%) of TVIE were related to Staphylococcus aureus and 4/29 (13.8%) were secondary to fungal infection. During a follow-up of 5.4 ± 3.7 years, there were 9 (34.6%) deaths and 15 (57.7%) composite outcomes. Multivariable Cox regression analysis showed that male sex (hazard ratio [HR]: 16.68, 95% confidence interval [CI]: 1.63-170.34, p = 0.018) and intravenous drug users (IVDU) (HR: 25.66, 95% CI: 1.87-352.79, p = 0.015) are significantly associated with increase death; on the other hand, higher level of preoperative hemoglobin and preoperative left ventricular ejection fraction (LVEF) was found to have decreased hazard of death: HR: 0.90, 95% CI: 0.82-0.99, p = 0.033 and HR: 0.92, 95% CI: 0.86-0.98, p = 0.013, respectively.
Conclusion: In our institution, surgical intervention for isolated TVIE has a mortality rate of 34.6%. Men, a history of IVDU, lower preoperative hemoglobin levels, and reduced LVEF were significant predictors of postsurgical mortality. Earlier surgical intervention for TVIE before the development of anemia or impaired LV systolic function may have a potential survival benefit.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


