{"title":"Enhanced Recovery after Pediatric Cardiac Surgery: A Meta-Analysis.","authors":"Osama Abu-Shawer, Abdel-Rahman E'mar, Abdel-Rahman Jaber, Shatha Tailakh, Amer Abu-Shawer, Caroline Al-Haddadin","doi":"10.1055/s-0045-1808072","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Enhanced Recovery After Surgery (ERAS) protocols are a set of steps taken before, during, and after surgery to improve patient care and outcomes. While ERAS is well known for its benefits in various surgeries, its application in pediatric cardiac surgery is relatively new. With the recent emergence of studies on its implementation in pediatric cardiac surgery, this study is the first to systematically review the current evidence on the efficacy of ERAS in the field.</p><p><strong>Methods: </strong>A meta-analysis was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two reviewers independently searched PubMed, Cochrane, Google Scholar, Web of Science, Embase, and Scopus databases for comparative studies with control groups that described the use of ERAS in all types of pediatric cardiac surgeries from 2000 to 2024. The data collected included study design, patient demographics, elements of the ERAS protocols, and postoperative outcomes. The random-effects model was used to calculate the pooled odds ratios (ORs) and mean differences (MDs) with the corresponding confidence intervals (CIs) for proportional and continuous variables, respectively.</p><p><strong>Results: </strong>Five studies, involving 1,008 patients, were included in the final analysis: three randomized controlled trials (RCTs), one retrospective cohort, and one case-control study. The ERAS protocols were applied in 430 (43%) patients, and standard perioperative care was applied in 578 (57%) patients. The analysis revealed that implementing the ERAS protocol significantly reduced ICU length of stay ( <i>I</i> <sup>2</sup> = 98.26%; MD = -1.441; 95% CI: -2.610 to -0.273; <i>p</i> = 0.016). The ERAS group had a comparable rate of postoperative complications to the standard care group ( <i>I</i> <sup>2</sup> = 15.3%; OR: 0.889; 95% CI: 0.622-1.269; <i>p</i> = 0.516).</p><p><strong>Conclusions: </strong>The ERAS protocols in pediatric cardiac surgery appear to be safe and effective in improving certain short-term outcomes. However, evidence is limited due to the small number of studies. Further multicenter RCTs that fully incorporate the ERAS protocol elements and assess both immediate and long-term outcomes are needed.</p>","PeriodicalId":32889,"journal":{"name":"Avicenna Journal of Medicine","volume":"15 2","pages":"80-85"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178667/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Avicenna Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1808072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Enhanced Recovery After Surgery (ERAS) protocols are a set of steps taken before, during, and after surgery to improve patient care and outcomes. While ERAS is well known for its benefits in various surgeries, its application in pediatric cardiac surgery is relatively new. With the recent emergence of studies on its implementation in pediatric cardiac surgery, this study is the first to systematically review the current evidence on the efficacy of ERAS in the field.
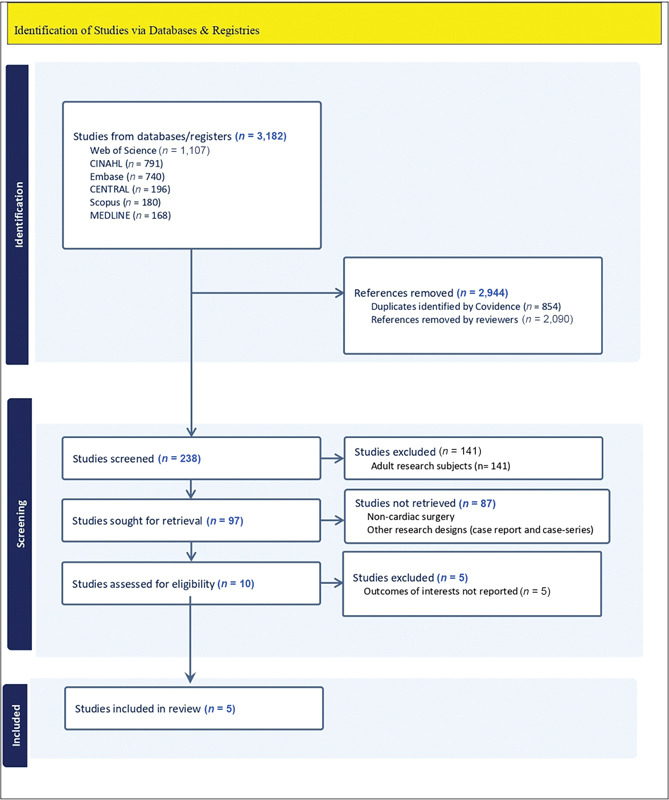
Methods: A meta-analysis was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two reviewers independently searched PubMed, Cochrane, Google Scholar, Web of Science, Embase, and Scopus databases for comparative studies with control groups that described the use of ERAS in all types of pediatric cardiac surgeries from 2000 to 2024. The data collected included study design, patient demographics, elements of the ERAS protocols, and postoperative outcomes. The random-effects model was used to calculate the pooled odds ratios (ORs) and mean differences (MDs) with the corresponding confidence intervals (CIs) for proportional and continuous variables, respectively.
Results: Five studies, involving 1,008 patients, were included in the final analysis: three randomized controlled trials (RCTs), one retrospective cohort, and one case-control study. The ERAS protocols were applied in 430 (43%) patients, and standard perioperative care was applied in 578 (57%) patients. The analysis revealed that implementing the ERAS protocol significantly reduced ICU length of stay ( I2 = 98.26%; MD = -1.441; 95% CI: -2.610 to -0.273; p = 0.016). The ERAS group had a comparable rate of postoperative complications to the standard care group ( I2 = 15.3%; OR: 0.889; 95% CI: 0.622-1.269; p = 0.516).
Conclusions: The ERAS protocols in pediatric cardiac surgery appear to be safe and effective in improving certain short-term outcomes. However, evidence is limited due to the small number of studies. Further multicenter RCTs that fully incorporate the ERAS protocol elements and assess both immediate and long-term outcomes are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


