Mary L Forte, Sallee Brandt, Amy Marie Claussen, Christopher J Tignanelli, Surbhi Shah, Mary Butler
{"title":"Venous thromboembolism prophylaxis in adults with acute traumatic brain injury: a systematic review.","authors":"Mary L Forte, Sallee Brandt, Amy Marie Claussen, Christopher J Tignanelli, Surbhi Shah, Mary Butler","doi":"10.1136/tsaco-2024-001691","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal timing and type of venous thromboembolism chemoprophylaxis (VTEp) for adults with acute traumatic brain injury (TBI) remains unknown. This systematic review synthesized evidence on the timing and type of VTEp in adults with TBI and highlights evidence gaps.</p><p><strong>Methods: </strong>We searched Ovid MEDLINE, Embase, and the Cochrane Library through November 4, 2024 for English language, randomized or non-randomized studies with a comparator that reported VTEp timing or agent in adults with acute TBI, and reported intracranial hemorrhage progression (ICHP), VTE, pulmonary embolism (PE), deep vein thrombosis (DVT), neurosurgical intervention (NSI), adverse events (AEs), length of stay (LOS), function, or mortality. Risk of bias (ROB) was assessed with ROBINS-I as low, moderate, serious, or critical risk in studies that used advanced analytic methods (AAMs) to control selection bias; all other studies were deemed critical risk. We qualitatively synthesized evidence and focused text reporting on studies with AAM.</p><p><strong>Results: </strong>From 738 citations, 21 non-randomized studies met criteria (1 moderate, 20 critical ROB): 16 on VTEp timing, 7 on agents. Seven studies used AAM. For VTEp timing (five AAM studies), one study of adults with mostly mild TBI found no significant difference between Early and Late VTEp on ICHP (moderate ROB); no timing studies with AAM reported ICHP for adults with moderate or severe TBI. Findings were mixed for VTE timing on NSI and PE. Early VTEp was associated with fewer DVTs. There was no difference in mortality or serious AEs by VTEp timing. For VTEp agents, three studies with AAM found no significant difference between low molecular weight heparin (LMWH) and unfractionated heparin (UH) on ICHP, PE, DVT, and serious or overall AEs. Results were mixed for LMWH versus UH effects on NSI after VTEp, VTE, LOS and mortality. TBI severity labeling varied across studies and within measures, reducing comparability.</p><p><strong>Conclusions: </strong>Clinical evidence on the timing and type of VTEp for adults with acute TBI is of insufficient quality for clinical decision-making. Prospective research designs, standardization of TBI severity labeling, and improved reporting of interventions and outcomes would advance the field.</p><p><strong>Prospero registration number: </strong>CRD42023421534.</p><p><strong>Level of evidence: </strong>Systematic Review, Level IV.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"10 2","pages":"e001691"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12184397/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001691","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal timing and type of venous thromboembolism chemoprophylaxis (VTEp) for adults with acute traumatic brain injury (TBI) remains unknown. This systematic review synthesized evidence on the timing and type of VTEp in adults with TBI and highlights evidence gaps.
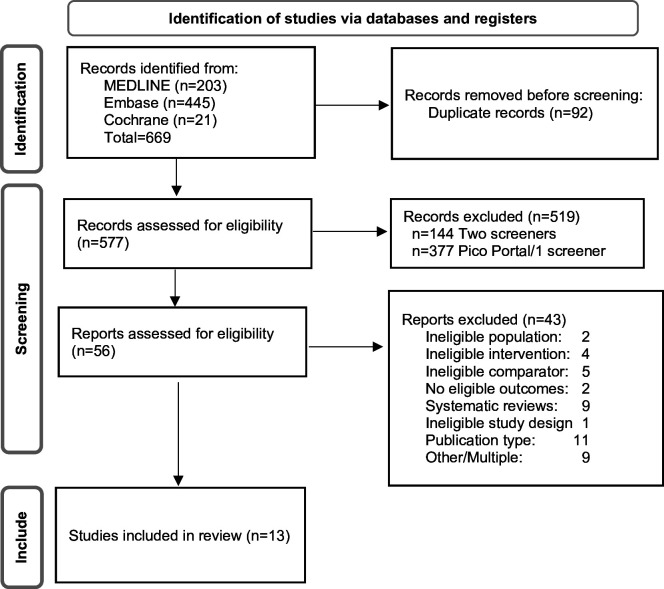
Methods: We searched Ovid MEDLINE, Embase, and the Cochrane Library through November 4, 2024 for English language, randomized or non-randomized studies with a comparator that reported VTEp timing or agent in adults with acute TBI, and reported intracranial hemorrhage progression (ICHP), VTE, pulmonary embolism (PE), deep vein thrombosis (DVT), neurosurgical intervention (NSI), adverse events (AEs), length of stay (LOS), function, or mortality. Risk of bias (ROB) was assessed with ROBINS-I as low, moderate, serious, or critical risk in studies that used advanced analytic methods (AAMs) to control selection bias; all other studies were deemed critical risk. We qualitatively synthesized evidence and focused text reporting on studies with AAM.
Results: From 738 citations, 21 non-randomized studies met criteria (1 moderate, 20 critical ROB): 16 on VTEp timing, 7 on agents. Seven studies used AAM. For VTEp timing (five AAM studies), one study of adults with mostly mild TBI found no significant difference between Early and Late VTEp on ICHP (moderate ROB); no timing studies with AAM reported ICHP for adults with moderate or severe TBI. Findings were mixed for VTE timing on NSI and PE. Early VTEp was associated with fewer DVTs. There was no difference in mortality or serious AEs by VTEp timing. For VTEp agents, three studies with AAM found no significant difference between low molecular weight heparin (LMWH) and unfractionated heparin (UH) on ICHP, PE, DVT, and serious or overall AEs. Results were mixed for LMWH versus UH effects on NSI after VTEp, VTE, LOS and mortality. TBI severity labeling varied across studies and within measures, reducing comparability.
Conclusions: Clinical evidence on the timing and type of VTEp for adults with acute TBI is of insufficient quality for clinical decision-making. Prospective research designs, standardization of TBI severity labeling, and improved reporting of interventions and outcomes would advance the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


