Sabrina E Carro, Nicolas Gargurevich, Mert Sekmen, Srinivasan Suresh, Judith M Martin, Derek J Williams
{"title":"Evaluating the antibiotic spectrum index in a stewardship-focused clinical trial for childhood pneumonia.","authors":"Sabrina E Carro, Nicolas Gargurevich, Mert Sekmen, Srinivasan Suresh, Judith M Martin, Derek J Williams","doi":"10.1017/ice.2025.10208","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The antibiotic spectrum index (ASI) outcome quantifies antibiotic exposure based on spectrum of activity. Our objective was to examine ASI as an exploratory outcome in the context of a recent stewardship-focused, clinical trial in childhood pneumonia that originally used a binary guideline-concordant outcome.</p><p><strong>Design: </strong>Secondary analysis of a randomized clinical trial.</p><p><strong>Setting: </strong>Two tertiary pediatric hospitals.</p><p><strong>Methods: </strong>Encounters were randomly assigned to clinical decision support (CDS) or usual care treatment arm. The ASI was calculated by summing daily ASI scores for each unique antibiotic administered. It was evaluated as a continuous and ordinal measure: No Antibiotics (ASI = 0), Narrow (1-2), Intermediate (3-4), Broad (5-7), and Very Broad (≥8). Proportional odds regression modeled the ordinal ASI outcome in the first 24 hours by treatment arm and compared to the guideline-concordance outcome. Results were stratified by emergency department (ED) disposition. We also conducted a longitudinal, descriptive analysis of day-to-day ASI for those with in-hospital dispositions.</p><p><strong>Results: </strong>We included 1027 encounters, 549 (53%) were randomized to CDS and 478 (47%) usual care respectively. ASI Category did not differ by treatment arm overall (Odds Ratio: 0.88[95% Confidence Interval: 0.70,1.09]), which mirrored binary guideline-concordance. Mean ASI was lower for concordant encounters (2.1 vs 8.4, <i>P</i> < 0.001) and across all ED dispositions. In the longitudinal analysis, there were 1137 day-to-day ASI comparisons, with only 7% representing spectrum escalations.</p><p><strong>Conclusions: </strong>The ASI outcome yielded similar results to a dichotomous concordance outcome. However, ASI provided more granular insights into antibiotic prescribing, suggesting ASI may be a useful outcome measure in future stewardship-focused trials.</p>","PeriodicalId":13663,"journal":{"name":"Infection Control and Hospital Epidemiology","volume":" ","pages":"1-7"},"PeriodicalIF":2.9000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12483619/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection Control and Hospital Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1017/ice.2025.10208","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The antibiotic spectrum index (ASI) outcome quantifies antibiotic exposure based on spectrum of activity. Our objective was to examine ASI as an exploratory outcome in the context of a recent stewardship-focused, clinical trial in childhood pneumonia that originally used a binary guideline-concordant outcome.
Design: Secondary analysis of a randomized clinical trial.
Setting: Two tertiary pediatric hospitals.
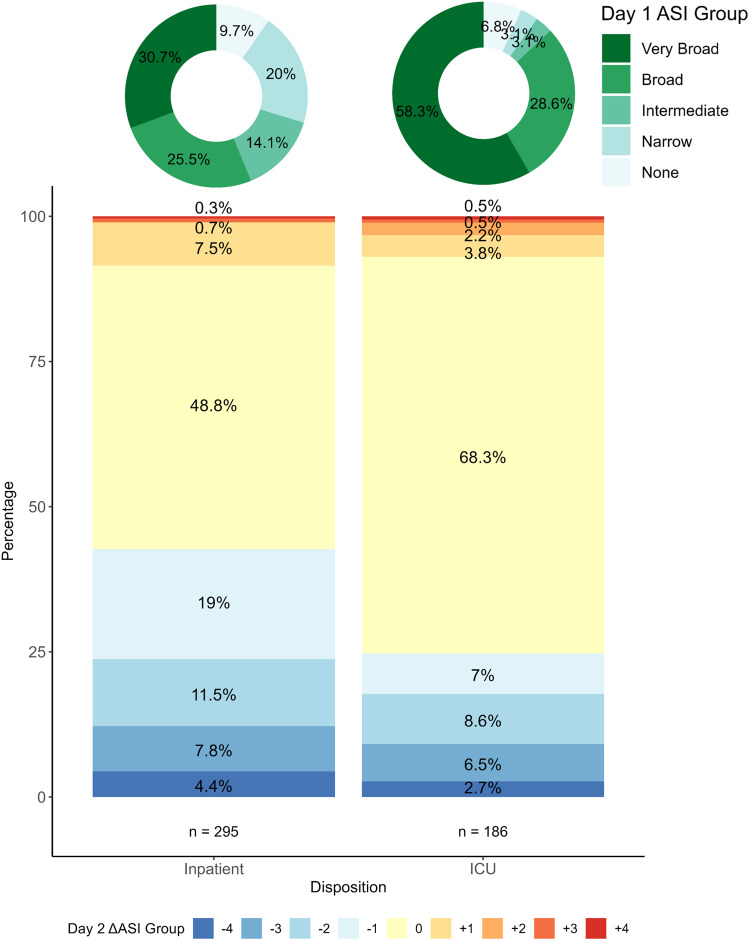
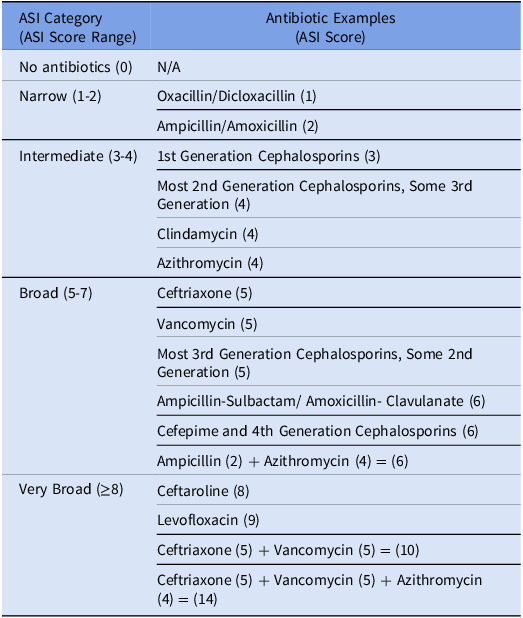
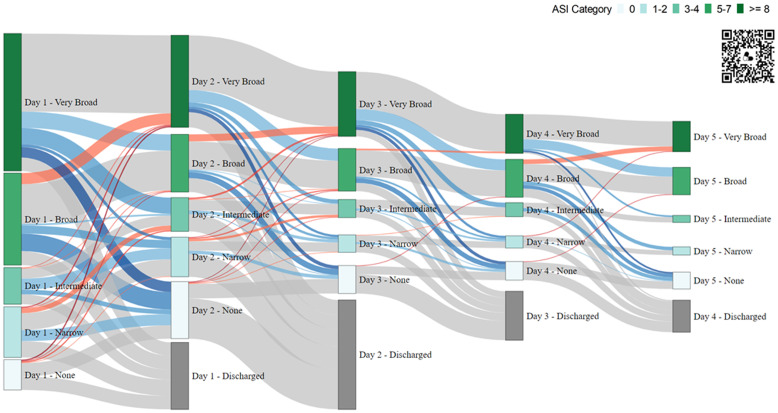
Methods: Encounters were randomly assigned to clinical decision support (CDS) or usual care treatment arm. The ASI was calculated by summing daily ASI scores for each unique antibiotic administered. It was evaluated as a continuous and ordinal measure: No Antibiotics (ASI = 0), Narrow (1-2), Intermediate (3-4), Broad (5-7), and Very Broad (≥8). Proportional odds regression modeled the ordinal ASI outcome in the first 24 hours by treatment arm and compared to the guideline-concordance outcome. Results were stratified by emergency department (ED) disposition. We also conducted a longitudinal, descriptive analysis of day-to-day ASI for those with in-hospital dispositions.
Results: We included 1027 encounters, 549 (53%) were randomized to CDS and 478 (47%) usual care respectively. ASI Category did not differ by treatment arm overall (Odds Ratio: 0.88[95% Confidence Interval: 0.70,1.09]), which mirrored binary guideline-concordance. Mean ASI was lower for concordant encounters (2.1 vs 8.4, P < 0.001) and across all ED dispositions. In the longitudinal analysis, there were 1137 day-to-day ASI comparisons, with only 7% representing spectrum escalations.
Conclusions: The ASI outcome yielded similar results to a dichotomous concordance outcome. However, ASI provided more granular insights into antibiotic prescribing, suggesting ASI may be a useful outcome measure in future stewardship-focused trials.
目的:抗生素谱指数(ASI)结果根据活性谱量化抗生素暴露。我们的目的是在最近一项以管理为重点的儿童肺炎临床试验的背景下,将ASI作为一项探索性结果进行研究,该试验最初使用二元指南一致性结果。设计:随机临床试验的二次分析。环境:两所三级儿科医院。方法:受试者被随机分配到临床决策支持组(CDS)或常规护理治疗组。ASI的计算方法是将每一种抗生素的每日ASI评分相加。以连续和有序的指标进行评估:无抗生素(ASI = 0),窄(1-2),中级(3-4),宽(5-7)和非常宽(≥8)。比例赔率回归模拟了治疗组前24小时的顺序ASI结果,并与指南一致性结果进行了比较。结果按急诊科(ED)处置分层。我们还对那些有住院倾向的患者进行了日常ASI的纵向描述性分析。结果:我们纳入1027例就诊,549例(53%)随机分配到CDS组,478例(47%)随机分配到常规护理组。总体而言,ASI类别在治疗组之间没有差异(优势比:0.88[95%置信区间:0.70,1.09]),这反映了二元指南一致性。和谐遭遇的平均ASI较低(2.1 vs 8.4, P < 0.001),所有ED处置的平均ASI较低。在纵向分析中,有1137个日常ASI比较,只有7%代表频谱升级。结论:ASI结果与二分类一致性结果相似。然而,ASI为抗生素处方提供了更细致的见解,这表明ASI可能是未来以管理为重点的试验中有用的结果衡量标准。
期刊介绍:
Infection Control and Hospital Epidemiology provides original, peer-reviewed scientific articles for anyone involved with an infection control or epidemiology program in a hospital or healthcare facility. Written by infection control practitioners and epidemiologists and guided by an editorial board composed of the nation''s leaders in the field, ICHE provides a critical forum for this vital information.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


