Laminectomy with fusion for cervical spondylotic myelopathy is associated with higher early morbidity and risk of perioperative complications compared with laminectomy alone: a retrospective study in the United States.
Abhinav Sharma, Paramveer Birring, Nischal Acharya, Manaav Mehta, Nicole Goldenhersh, Michael Steinhaus, Zorica Buser, Hao-Hua Wu, Sohaib Hashmi, Don Young Park, Yu-Po Lee, Nitin Bhatia
{"title":"Laminectomy with fusion for cervical spondylotic myelopathy is associated with higher early morbidity and risk of perioperative complications compared with laminectomy alone: a retrospective study in the United States.","authors":"Abhinav Sharma, Paramveer Birring, Nischal Acharya, Manaav Mehta, Nicole Goldenhersh, Michael Steinhaus, Zorica Buser, Hao-Hua Wu, Sohaib Hashmi, Don Young Park, Yu-Po Lee, Nitin Bhatia","doi":"10.31616/asj.2024.0350","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>A retrospective cohort study.</p><p><strong>Purpose: </strong>We present data assessing the differences in 30-day morbidity, mortality, and postoperative complications between the two surgical remedy options.</p><p><strong>Overview of literature: </strong>The choice between decompression with fusion or decompression alone for the management of cervical spondylotic myelopathy (CSM) remains controversial.</p><p><strong>Methods: </strong>The American College of Surgeons National Quality Improvement Program database was queried for adults ≥18 years diagnosed with spondylosis with cervical myelopathy (10th revision of the International Classification of Diseases [ICD-10]: M47.12) or spinal stenosis of the cervical region (ICD-10: M48.02) who underwent laminectomy (Current Procedural Terminology [CPT] 63001, 63015, 63045) with or without fusion (CPT 22600) between 2015 and 2020. Patients were stratified into fusion and non-fusion cohorts for comparative review. Estimated 30-day mortality and morbidity, postoperative complications, and American Society of Anesthesiologists (ASA) classification were evaluated using chi-square and analysis of variance tests, and results were further stratified according to ASA classification.</p><p><strong>Results: </strong>Of the 6,412 patients, 3,355 (52%) received laminectomy without fusion, and 3,057 (48%) experienced laminectomy with fusion. Patients undergoing decompression with fusion had higher mean morbidity (estimated probability 0.073 vs. 0.064, p<0.001), unplanned reoperations (4.2% vs. 2.7%, p<0.002), unplanned readmissions (7.6% vs. 6.3%, p<0.014), mean length of stay (5.0±8.9 days vs. 3.4±7.2 days, p<0.001), deep wound infections (0.8% vs. 0.4%, p<0.022), and bleeding risk necessitating transfusion (3.8% vs. 1.6%, p<0.001). Stratification by ASA scores demonstrated an overall higher rate of 30-day postoperative complications with increasing ASA scores in both cohorts, However, the decompression with fusion cohort showed a greater relative increase in complications compared to the decompression-alone cohort with each ASA group.</p><p><strong>Conclusions: </strong>Decompression with fusion is correlated with higher estimated morbidity, unplanned reoperations and readmissions, and 30-day complications postoperatively. Decompression alone is an appealing procedure option for CSM, particularly for patients with higher ASA scores and those at greater risk.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"507-515"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400103/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2024.0350","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: A retrospective cohort study.
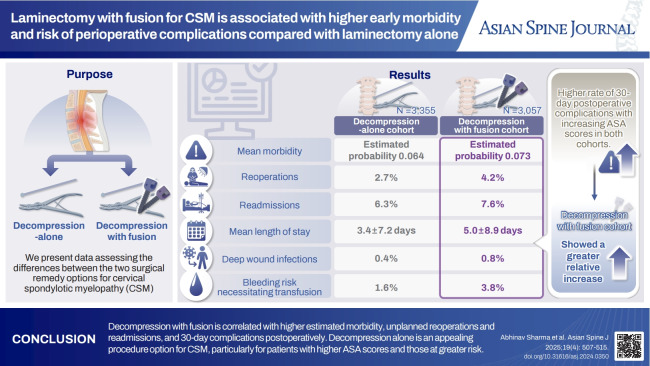
Purpose: We present data assessing the differences in 30-day morbidity, mortality, and postoperative complications between the two surgical remedy options.
Overview of literature: The choice between decompression with fusion or decompression alone for the management of cervical spondylotic myelopathy (CSM) remains controversial.
Methods: The American College of Surgeons National Quality Improvement Program database was queried for adults ≥18 years diagnosed with spondylosis with cervical myelopathy (10th revision of the International Classification of Diseases [ICD-10]: M47.12) or spinal stenosis of the cervical region (ICD-10: M48.02) who underwent laminectomy (Current Procedural Terminology [CPT] 63001, 63015, 63045) with or without fusion (CPT 22600) between 2015 and 2020. Patients were stratified into fusion and non-fusion cohorts for comparative review. Estimated 30-day mortality and morbidity, postoperative complications, and American Society of Anesthesiologists (ASA) classification were evaluated using chi-square and analysis of variance tests, and results were further stratified according to ASA classification.
Results: Of the 6,412 patients, 3,355 (52%) received laminectomy without fusion, and 3,057 (48%) experienced laminectomy with fusion. Patients undergoing decompression with fusion had higher mean morbidity (estimated probability 0.073 vs. 0.064, p<0.001), unplanned reoperations (4.2% vs. 2.7%, p<0.002), unplanned readmissions (7.6% vs. 6.3%, p<0.014), mean length of stay (5.0±8.9 days vs. 3.4±7.2 days, p<0.001), deep wound infections (0.8% vs. 0.4%, p<0.022), and bleeding risk necessitating transfusion (3.8% vs. 1.6%, p<0.001). Stratification by ASA scores demonstrated an overall higher rate of 30-day postoperative complications with increasing ASA scores in both cohorts, However, the decompression with fusion cohort showed a greater relative increase in complications compared to the decompression-alone cohort with each ASA group.
Conclusions: Decompression with fusion is correlated with higher estimated morbidity, unplanned reoperations and readmissions, and 30-day complications postoperatively. Decompression alone is an appealing procedure option for CSM, particularly for patients with higher ASA scores and those at greater risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


