Impact of awake prone positioning duration on intubation or mortality in COVID-19 patients with acute respiratory failure: secondary analysis of a randomized clinical trial.
{"title":"Impact of awake prone positioning duration on intubation or mortality in COVID-19 patients with acute respiratory failure: secondary analysis of a randomized clinical trial.","authors":"Qin Sun, Rui Zhang, Junyi Zhang, Jianfeng Xie, Yingzi Huang, Yi Yang, Haibo Qiu, Ling Liu, Hui Chen","doi":"10.1186/s13613-025-01501-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Compared with shorter awake prone positioning (APP), prolonged APP (≥ 12 h daily) reduces the intubation rate in patients with COVID-19-related acute hypoxemic respiratory failure (AHRF). However, the optimal APP duration is uncertain. In this secondary analysis, we aimed to explore whether a longer APP duration is associated with improved outcomes and to identify the optimal duration of APP.</p><p><strong>Methods: </strong>Data from a multicenter randomized controlled trial involving nonintubated COVID-19 patients with AHRF were analyzed. Daily APP duration over 7 days after randomization was recorded as the primary exposure in present study. The primary outcome was the time from randomization to APP failure, which was defined as a composite of tracheal intubation or mortality within 28 days. A Cox proportional hazards regression model was employed to elucidate the associations, and the daily duration of APP was treated as time dependent.</p><p><strong>Results: </strong>A total of 409 patients were randomized in the original trial, and 408 were enrolled in this analysis. Among these patients, 105 (25.7%) experienced APP failure. A longer daily APP duration was associated with a lower risk of APP failure, with a hazard ratio (HR) of 0.93 (95% confidence interval (CI): 0.88-0.98), and the association was significant only during the first three days after randomization. There was a nonlinear relationship between the daily APP duration and the risk of APP failure (P = 0.015 for nonlinearity). Compared with patients whose APP duration ranged from 8 to 12 h per day, patients with less than 8 h of APP per day had a greater risk of APP failure (HR 2.44, 95% CI 1.21-4.92), whereas extending APP beyond 12 h per day did not improve the outcomes further (HR 1.03, 95% CI 0.51-2.10, P = 0.932).</p><p><strong>Interpretation: </strong>A longer daily APP duration was associated with a reduced risk of APP failure in COVID-19-related AHRF patients, and the optimal APP duration was 8-12 h per day. Clinical trial ClinicalTrials.gov: NCT05677984, Registered January 3, 2023. https://register.</p><p><strong>Clinicaltrials: </strong>gov/prs/app/action/SelectProtocol?sid=S000CST9&selectaction=Edit&uid=U0000YKY&ts=4&cx=-x0muek.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"84"},"PeriodicalIF":5.5000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185815/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01501-8","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Compared with shorter awake prone positioning (APP), prolonged APP (≥ 12 h daily) reduces the intubation rate in patients with COVID-19-related acute hypoxemic respiratory failure (AHRF). However, the optimal APP duration is uncertain. In this secondary analysis, we aimed to explore whether a longer APP duration is associated with improved outcomes and to identify the optimal duration of APP.
Methods: Data from a multicenter randomized controlled trial involving nonintubated COVID-19 patients with AHRF were analyzed. Daily APP duration over 7 days after randomization was recorded as the primary exposure in present study. The primary outcome was the time from randomization to APP failure, which was defined as a composite of tracheal intubation or mortality within 28 days. A Cox proportional hazards regression model was employed to elucidate the associations, and the daily duration of APP was treated as time dependent.
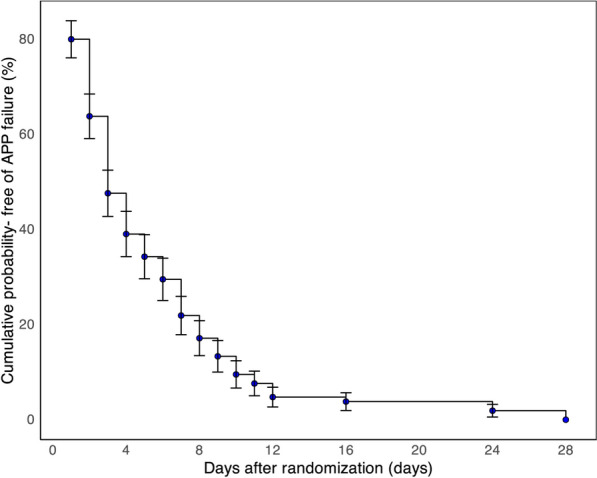
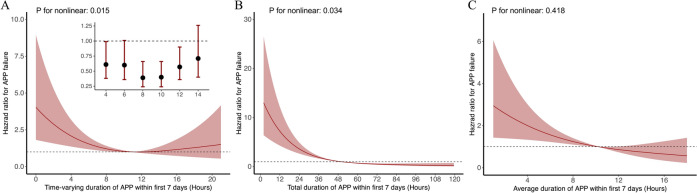
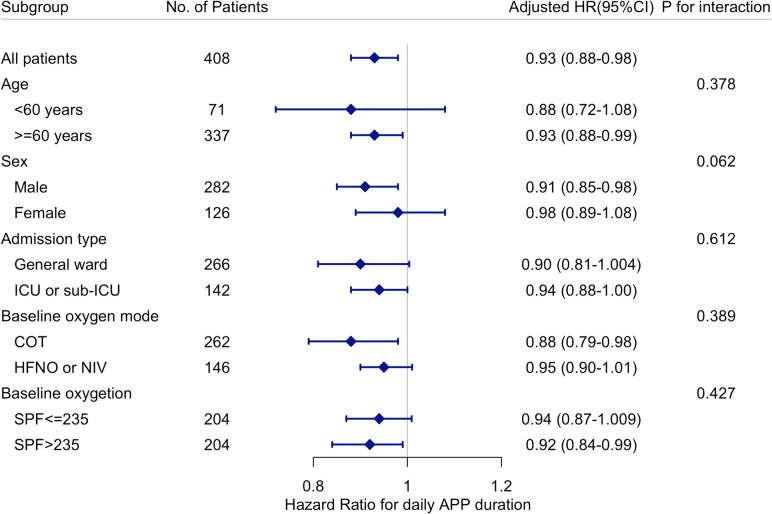
Results: A total of 409 patients were randomized in the original trial, and 408 were enrolled in this analysis. Among these patients, 105 (25.7%) experienced APP failure. A longer daily APP duration was associated with a lower risk of APP failure, with a hazard ratio (HR) of 0.93 (95% confidence interval (CI): 0.88-0.98), and the association was significant only during the first three days after randomization. There was a nonlinear relationship between the daily APP duration and the risk of APP failure (P = 0.015 for nonlinearity). Compared with patients whose APP duration ranged from 8 to 12 h per day, patients with less than 8 h of APP per day had a greater risk of APP failure (HR 2.44, 95% CI 1.21-4.92), whereas extending APP beyond 12 h per day did not improve the outcomes further (HR 1.03, 95% CI 0.51-2.10, P = 0.932).
Interpretation: A longer daily APP duration was associated with a reduced risk of APP failure in COVID-19-related AHRF patients, and the optimal APP duration was 8-12 h per day. Clinical trial ClinicalTrials.gov: NCT05677984, Registered January 3, 2023. https://register.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


