Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning.
Andreas F Dalen, Martin G Gregersen, Aleksander L Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A Nilsen, Marius Molund
{"title":"Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning.","authors":"Andreas F Dalen, Martin G Gregersen, Aleksander L Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A Nilsen, Marius Molund","doi":"10.1177/10711007251334085","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Weber B (supination external rotation) ankle fractures with complete deltoid ligament rupture (SER4b) are typically considered unstable and treated with plate fixation of the fibula. Recent studies have suggested a significant ankle-stabilizing role of the deep posterior tibiotalar ligament (dPTTL), which questions current practice. To our knowledge, there are few studies on the biomechanical effects of plate fixation and none on dPTTL repair. Therefore, this study aims to evaluate the effects of fibular plate fixation and dPTTL repair on ankle stability in a Weber B fracture model with complete deltoid ligament sectioning.</p><p><strong>Methods: </strong>We robotically tested 15 cadaveric ankle specimens in 5 states: native joint, SER4b injury models, SER4b injury models with plate fixation of the fibula, SER4b injury models with dPTTL repair, and SER4b injury models with combined plate fixation and dPTTL repair. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation. Talar shift and talar tilt were measured on mortise view radiographs. The primary outcome was differences in talar shift in neutral ankle position.</p><p><strong>Results: </strong>When comparing SER4b injury models with plate fixation to native ankles, we found a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, <i>P</i> ≤ .001), talar tilt of 14.47 degrees (95% CI 12.90-16.05, <i>P</i> ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, <i>P</i> ≤ .001). When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, we found a mean difference in talar shift of 0.23 mm (95% CI -0.07 to 0.54, <i>P</i> = .132), talar tilt of 1.65 degrees (95% CI 0.07-3.22, <i>P</i> = .040), and external rotation of 5.26 degrees (95% CI 2.82-7.70, <i>P</i> ≤ .001).</p><p><strong>Conclusion: </strong>This study's main finding was that plate fixation of the fibula alone did not considerably enhance ankle stability in SER4b injury models. However, ankle stability was substantially improved when plate fixation and dPTTL repair were combined.</p><p><strong>Clinical relevance: </strong>Our study showed that dPTTL repair, in addition to plate fixation, improved ankle stability in Weber B SER4b fracture models. This information should be considered in future clinical research and treatment strategies for these fractures.</p>","PeriodicalId":94011,"journal":{"name":"Foot & ankle international","volume":" ","pages":"688-696"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227801/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & ankle international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/10711007251334085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Weber B (supination external rotation) ankle fractures with complete deltoid ligament rupture (SER4b) are typically considered unstable and treated with plate fixation of the fibula. Recent studies have suggested a significant ankle-stabilizing role of the deep posterior tibiotalar ligament (dPTTL), which questions current practice. To our knowledge, there are few studies on the biomechanical effects of plate fixation and none on dPTTL repair. Therefore, this study aims to evaluate the effects of fibular plate fixation and dPTTL repair on ankle stability in a Weber B fracture model with complete deltoid ligament sectioning.
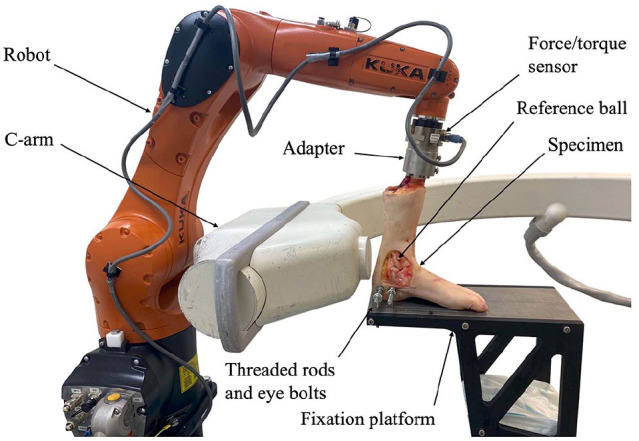
Methods: We robotically tested 15 cadaveric ankle specimens in 5 states: native joint, SER4b injury models, SER4b injury models with plate fixation of the fibula, SER4b injury models with dPTTL repair, and SER4b injury models with combined plate fixation and dPTTL repair. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation. Talar shift and talar tilt were measured on mortise view radiographs. The primary outcome was differences in talar shift in neutral ankle position.
Results: When comparing SER4b injury models with plate fixation to native ankles, we found a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, P ≤ .001), talar tilt of 14.47 degrees (95% CI 12.90-16.05, P ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, P ≤ .001). When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, we found a mean difference in talar shift of 0.23 mm (95% CI -0.07 to 0.54, P = .132), talar tilt of 1.65 degrees (95% CI 0.07-3.22, P = .040), and external rotation of 5.26 degrees (95% CI 2.82-7.70, P ≤ .001).
Conclusion: This study's main finding was that plate fixation of the fibula alone did not considerably enhance ankle stability in SER4b injury models. However, ankle stability was substantially improved when plate fixation and dPTTL repair were combined.
Clinical relevance: Our study showed that dPTTL repair, in addition to plate fixation, improved ankle stability in Weber B SER4b fracture models. This information should be considered in future clinical research and treatment strategies for these fractures.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


