Cristina Ghadban, Mayte García-Unzueta, Juan Agüero, Paula Martín-Audera, Bernardo Alio Lavín, Armando Raúl Guerra, Ana Berja, Nieves Aranda, Anastasia Guzun, Ana Isabel Insua, Carlos Antonio Amado
{"title":"Associations between serum levels of ferroptosis-related molecules and outcomes in stable COPD: an exploratory prospective observational study.","authors":"Cristina Ghadban, Mayte García-Unzueta, Juan Agüero, Paula Martín-Audera, Bernardo Alio Lavín, Armando Raúl Guerra, Ana Berja, Nieves Aranda, Anastasia Guzun, Ana Isabel Insua, Carlos Antonio Amado","doi":"10.1007/s11739-025-04016-z","DOIUrl":null,"url":null,"abstract":"<p><p>Ferroptosis is an iron-dependent form of cell death that contributes to the pathophysiology of chronic obstructive pulmonary disease (COPD). Ferroptosis-associated factors, including acyl-CoA synthetase long-chain family 4 (ACSL4), soluble transferrin receptor 1 (sTfR1), glutathione peroxidase 4 (GPX4), and apoptosis-inducing factor 2, (AIFM2) mediate intracellular iron metabolism, oxidative stress, and lipid peroxidation. Despite their potential clinical relevance, no studies have measured serum levels of these factors with respect to the manifestations of COPD. The study enrolled 179 stable, non-anemic outpatients diagnosed with COPD and 57 age- and sex-matched smokers who did not carry this diagnosis. Clinical characteristics were assessed together with baseline serum levels of the four ferroptosis-associated factors. Moderate and severe exacerbations of COPD were monitored over the following 12 months. Soluble TfR1 levels were higher and GPX4 levels were lower among those in the COPD group compared to smokers without COPD (p = 0.004 and p = 0.002, respectively). The sTfR1/GPX4 ratio was also higher among those in the COPD group (p = 0.001). Multivariate analysis identified low serum GPX4 (OR 5.475; p = 0.001), and high sTfR1/GPX4 (OR 4.293; p < 0.001) as independent predictors of poor performance on the six-minute walk distance test. Additionally, high sTfR1 (HR 1.850; p = 0.004), low GPX4 (HR 2.301; p = 0.001), and high sTfR1/GPX4 (HR 2.223; p < 0.001) were associated with increased risk of moderate exacerbation. High sTfR1 (HR 2.970; p = 0.014), low GPX4 (HR 3.753; p = 0.012), and high sTfR1/GPX4 (HR 3.668; p = 0.009) were also independent predictors of severe exacerbation. Serum levels of ferroptosis-associated factors were significantly different in patients diagnosed with COPD compared to smokers who had not been diagnosed with this disorder. Elevated sTfR1, low levels of GPX4, and higher sTfR1/GPX4 were associated with poor clinical outcomes, including reduced exercise capacity and an increased risk of moderate and severe exacerbations. These findings highlight the potential of ferroptosis-associated factors, particularly the calculated sTfR1/GPX4, in predicting COPD progression and the risk of exacerbation in stable, non-anemic outpatients.</p>","PeriodicalId":13662,"journal":{"name":"Internal and Emergency Medicine","volume":" ","pages":"1761-1773"},"PeriodicalIF":3.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476405/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Internal and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11739-025-04016-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
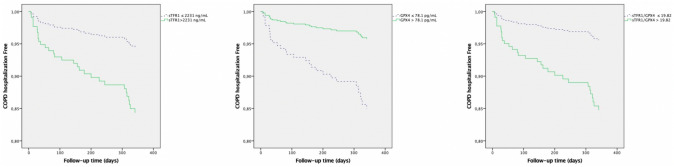
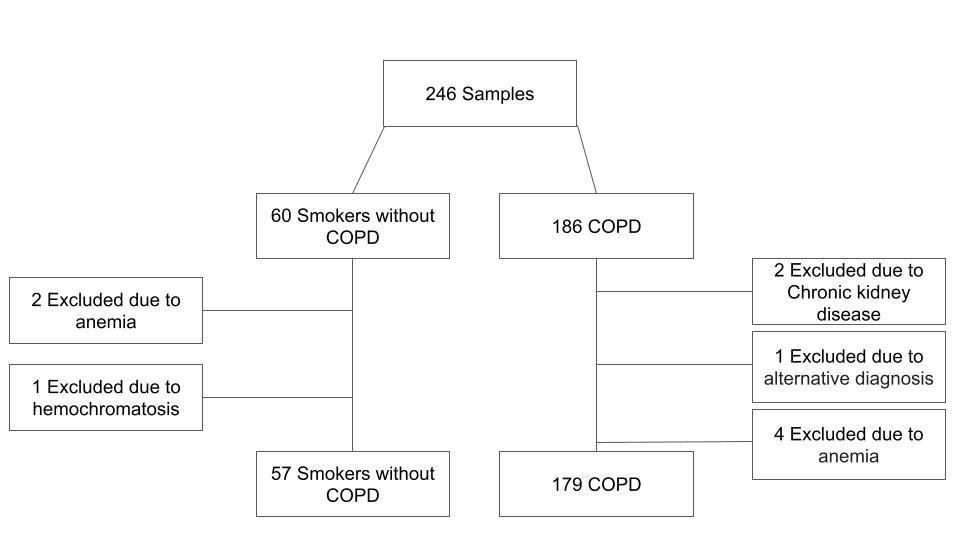
Ferroptosis is an iron-dependent form of cell death that contributes to the pathophysiology of chronic obstructive pulmonary disease (COPD). Ferroptosis-associated factors, including acyl-CoA synthetase long-chain family 4 (ACSL4), soluble transferrin receptor 1 (sTfR1), glutathione peroxidase 4 (GPX4), and apoptosis-inducing factor 2, (AIFM2) mediate intracellular iron metabolism, oxidative stress, and lipid peroxidation. Despite their potential clinical relevance, no studies have measured serum levels of these factors with respect to the manifestations of COPD. The study enrolled 179 stable, non-anemic outpatients diagnosed with COPD and 57 age- and sex-matched smokers who did not carry this diagnosis. Clinical characteristics were assessed together with baseline serum levels of the four ferroptosis-associated factors. Moderate and severe exacerbations of COPD were monitored over the following 12 months. Soluble TfR1 levels were higher and GPX4 levels were lower among those in the COPD group compared to smokers without COPD (p = 0.004 and p = 0.002, respectively). The sTfR1/GPX4 ratio was also higher among those in the COPD group (p = 0.001). Multivariate analysis identified low serum GPX4 (OR 5.475; p = 0.001), and high sTfR1/GPX4 (OR 4.293; p < 0.001) as independent predictors of poor performance on the six-minute walk distance test. Additionally, high sTfR1 (HR 1.850; p = 0.004), low GPX4 (HR 2.301; p = 0.001), and high sTfR1/GPX4 (HR 2.223; p < 0.001) were associated with increased risk of moderate exacerbation. High sTfR1 (HR 2.970; p = 0.014), low GPX4 (HR 3.753; p = 0.012), and high sTfR1/GPX4 (HR 3.668; p = 0.009) were also independent predictors of severe exacerbation. Serum levels of ferroptosis-associated factors were significantly different in patients diagnosed with COPD compared to smokers who had not been diagnosed with this disorder. Elevated sTfR1, low levels of GPX4, and higher sTfR1/GPX4 were associated with poor clinical outcomes, including reduced exercise capacity and an increased risk of moderate and severe exacerbations. These findings highlight the potential of ferroptosis-associated factors, particularly the calculated sTfR1/GPX4, in predicting COPD progression and the risk of exacerbation in stable, non-anemic outpatients.
期刊介绍:
Internal and Emergency Medicine (IEM) is an independent, international, English-language, peer-reviewed journal designed for internists and emergency physicians. IEM publishes a variety of manuscript types including Original investigations, Review articles, Letters to the Editor, Editorials and Commentaries. Occasionally IEM accepts unsolicited Reviews, Commentaries or Editorials. The journal is divided into three sections, i.e., Internal Medicine, Emergency Medicine and Clinical Evidence and Health Technology Assessment, with three separate editorial boards. In the Internal Medicine section, invited Case records and Physical examinations, devoted to underlining the role of a clinical approach in selected clinical cases, are also published. The Emergency Medicine section will include a Morbidity and Mortality Report and an Airway Forum concerning the management of difficult airway problems. As far as Critical Care is becoming an integral part of Emergency Medicine, a new sub-section will report the literature that concerns the interface not only for the care of the critical patient in the Emergency Department, but also in the Intensive Care Unit. Finally, in the Clinical Evidence and Health Technology Assessment section brief discussions of topics of evidence-based medicine (Cochrane’s corner) and Research updates are published. IEM encourages letters of rebuttal and criticism of published articles. Topics of interest include all subjects that relate to the science and practice of Internal and Emergency Medicine.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


