Open Access to Antipsychotics in State Medicaid Programs: Effect on Healthcare Resource Utilization and Costs among Patients with Serious Mental Illness.
Rashmi Patel, Onur Baser, Heidi C Waters, Daniel Huang, Leigh Morrissey, Katarzyna Rodchenko, Gabriela Samayoa
{"title":"Open Access to Antipsychotics in State Medicaid Programs: Effect on Healthcare Resource Utilization and Costs among Patients with Serious Mental Illness.","authors":"Rashmi Patel, Onur Baser, Heidi C Waters, Daniel Huang, Leigh Morrissey, Katarzyna Rodchenko, Gabriela Samayoa","doi":"10.36469/001c.137909","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The restrictive consequences of Medicaid formulary restriction policies on antipsychotic medications may lead to higher healthcare utilization and costs among beneficiaries with serious mental illness (SMI). <b>Objectives:</b> This study compared outcomes among patients with SMI accessing antipsychotic medications through state Medicaid programs with open access (OA) policies (Michigan) vs 5 states without Medicaid OA policies (California, Colorado, Florida, Illinois, Wisconsin). <b>Methods:</b> A retrospective analysis was conducted using Kythera Labs Medicaid data (Jan. 1, 2016-Dec. 31, 2023). Outcomes were assessed for patients with SMI (>18 years of age, ≥1 antipsychotic medication claim during the identification period (Jan. 1, 2017-Dec. 31, 2022), ≥1 SMI claim in the 12-month baseline). Continuous medical and pharmacy benefits were required for 12 months pre- and post-index date. Outcomes included SMI-related hospital admissions, length of hospital stay, emergency department and outpatient visits, and associated costs. <b>Results:</b> A greater proportion of beneficiaries with SMI resided in Michigan than in the other states. After matching, significantly more antipsychotics users experienced SMI-related hospitalizations in California (18.25% vs 9.47%, P < .0001), Colorado (11.41% vs 7.33%, P =.0004), Florida (19.70% vs 10.17%, P < .0001), Illinois (23.57% vs 8.79%, P < .0001), and Wisconsin (15.21% vs 10.02%, P = .0046) than in Michigan. Length of stay was lower in Michigan than in California, Colorado, and Illinois. Inpatient costs related to SMI were significantly lower in Michigan, yet pharmacy costs were higher. Total SMI-related costs were higher in all non-OA states than in Michigan, except Colorado. <b>Discussion:</b> State Medicaid programs without OA to antipsychotics were associated with higher rates of SMI-related resource utilization and costs vs Michigan. <b>Conclusions:</b> Policy makers should consider the potential downstream cost implications of restrictive access policies and evaluate whether OA could result in improved health outcomes for patients and savings for Medicaid programs.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 1","pages":"222-229"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178157/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.137909","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
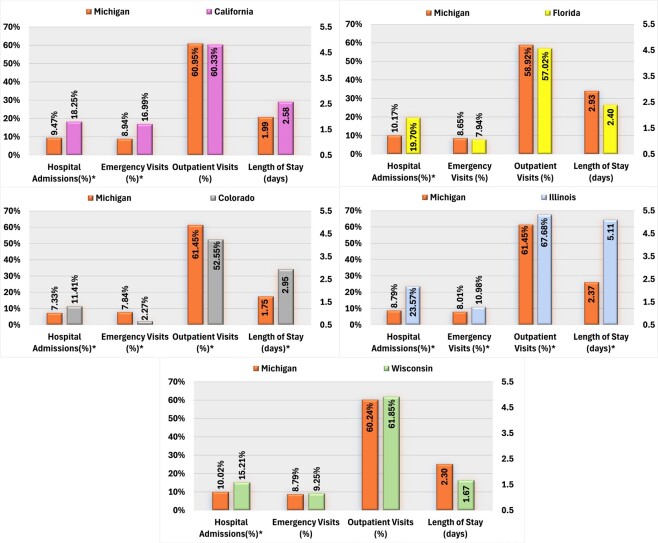
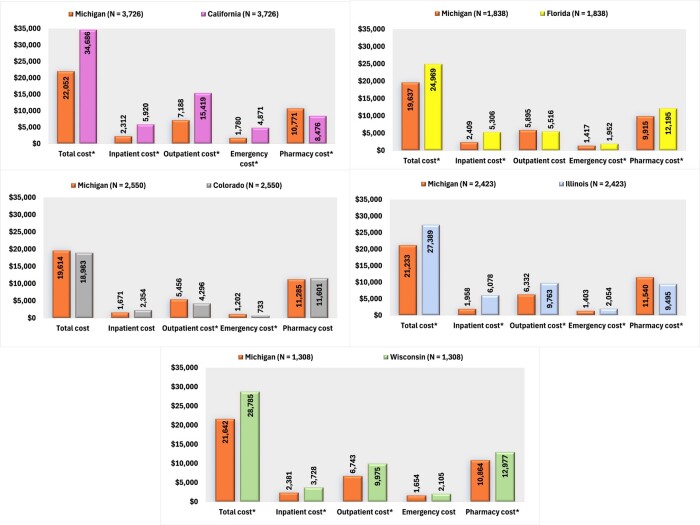
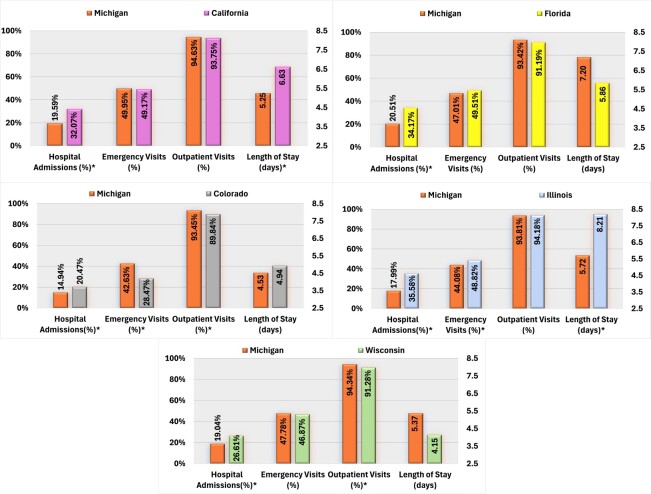
Background: The restrictive consequences of Medicaid formulary restriction policies on antipsychotic medications may lead to higher healthcare utilization and costs among beneficiaries with serious mental illness (SMI). Objectives: This study compared outcomes among patients with SMI accessing antipsychotic medications through state Medicaid programs with open access (OA) policies (Michigan) vs 5 states without Medicaid OA policies (California, Colorado, Florida, Illinois, Wisconsin). Methods: A retrospective analysis was conducted using Kythera Labs Medicaid data (Jan. 1, 2016-Dec. 31, 2023). Outcomes were assessed for patients with SMI (>18 years of age, ≥1 antipsychotic medication claim during the identification period (Jan. 1, 2017-Dec. 31, 2022), ≥1 SMI claim in the 12-month baseline). Continuous medical and pharmacy benefits were required for 12 months pre- and post-index date. Outcomes included SMI-related hospital admissions, length of hospital stay, emergency department and outpatient visits, and associated costs. Results: A greater proportion of beneficiaries with SMI resided in Michigan than in the other states. After matching, significantly more antipsychotics users experienced SMI-related hospitalizations in California (18.25% vs 9.47%, P < .0001), Colorado (11.41% vs 7.33%, P =.0004), Florida (19.70% vs 10.17%, P < .0001), Illinois (23.57% vs 8.79%, P < .0001), and Wisconsin (15.21% vs 10.02%, P = .0046) than in Michigan. Length of stay was lower in Michigan than in California, Colorado, and Illinois. Inpatient costs related to SMI were significantly lower in Michigan, yet pharmacy costs were higher. Total SMI-related costs were higher in all non-OA states than in Michigan, except Colorado. Discussion: State Medicaid programs without OA to antipsychotics were associated with higher rates of SMI-related resource utilization and costs vs Michigan. Conclusions: Policy makers should consider the potential downstream cost implications of restrictive access policies and evaluate whether OA could result in improved health outcomes for patients and savings for Medicaid programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


