Jared Walz, Glen Leverson, Lily Stalter, John Rice, David Al-Adra, Joshua J. Wiegel
{"title":"Impact of Direct-Acting Antiviral Therapy on Tacrolimus Pharmacokinetics in Hepatitis C Virus Nucleic Acid Testing-Positive Transplant Recipients","authors":"Jared Walz, Glen Leverson, Lily Stalter, John Rice, David Al-Adra, Joshua J. Wiegel","doi":"10.1155/jcpt/5727663","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Purpose:</b> Direct-acting antiviral agents (DAAs) against hepatitis C virus (HCV) such as sofosbuvir/velpatasvir (SOF/VEL) and glecaprevir/pibrentasvir (GLE/PIB) are effective in treating recipients of organs infected with HCV. The objective of this project is to identify changes in tacrolimus pharmacokinetics throughout DAA therapy in recipients of abdominal transplants from nucleic acid testing-positive (NAT+) donors.</p>\n <p><b>Methods:</b> Adult kidney or liver transplant recipients transplanted between 4/22/2019 and 6/23/2022 were included. Recipients of HCV NAT+ organs were treated with DAAs based on institutional protocol and insurance preference. Recipients of HCV NAT− organs from donors who fit Public Health Service (PHS) risk criteria for HCV transmission were included in the comparator group. Tacrolimus doses and concentrations were collected at DAA initiation and cessation and at the time of sustained virologic response assessment at 12 weeks after treatment completion (SVR12); these time points were matched in the NAT− control group. The primary outcome was difference in concentration-to-dose ratio (C/D) change (ΔC/D) over time between NAT+ and NAT− organ recipients.</p>\n <p><b>Results:</b> At DAA initiation, NAT+ organ recipients required a lower tacrolimus dose to reach goal than NAT− organ recipients (ΔC/D NAT+ = −0.41, ΔC/D NAT− 0.60, <i>p</i> = 0.01); however, a known tacrolimus interaction with fluconazole—administered to liver transplant recipients at high risk for invasive fungal infection (IFI)—represents a significant confounding factor. No differences in average C/D ratio between NAT+ and NAT− organ recipients were identified at any time point.</p>\n <p><b>Conclusion:</b> These results do not support empiric dose adjustments based on donor HCV NAT status or antiviral therapy.</p>\n </div>","PeriodicalId":15381,"journal":{"name":"Journal of Clinical Pharmacy and Therapeutics","volume":"2025 1","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/jcpt/5727663","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Pharmacy and Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/jcpt/5727663","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Direct-acting antiviral agents (DAAs) against hepatitis C virus (HCV) such as sofosbuvir/velpatasvir (SOF/VEL) and glecaprevir/pibrentasvir (GLE/PIB) are effective in treating recipients of organs infected with HCV. The objective of this project is to identify changes in tacrolimus pharmacokinetics throughout DAA therapy in recipients of abdominal transplants from nucleic acid testing-positive (NAT+) donors.
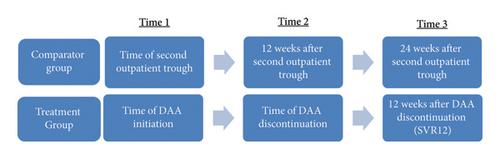
Methods: Adult kidney or liver transplant recipients transplanted between 4/22/2019 and 6/23/2022 were included. Recipients of HCV NAT+ organs were treated with DAAs based on institutional protocol and insurance preference. Recipients of HCV NAT− organs from donors who fit Public Health Service (PHS) risk criteria for HCV transmission were included in the comparator group. Tacrolimus doses and concentrations were collected at DAA initiation and cessation and at the time of sustained virologic response assessment at 12 weeks after treatment completion (SVR12); these time points were matched in the NAT− control group. The primary outcome was difference in concentration-to-dose ratio (C/D) change (ΔC/D) over time between NAT+ and NAT− organ recipients.
Results: At DAA initiation, NAT+ organ recipients required a lower tacrolimus dose to reach goal than NAT− organ recipients (ΔC/D NAT+ = −0.41, ΔC/D NAT− 0.60, p = 0.01); however, a known tacrolimus interaction with fluconazole—administered to liver transplant recipients at high risk for invasive fungal infection (IFI)—represents a significant confounding factor. No differences in average C/D ratio between NAT+ and NAT− organ recipients were identified at any time point.
Conclusion: These results do not support empiric dose adjustments based on donor HCV NAT status or antiviral therapy.
期刊介绍:
The Journal of Clinical Pharmacy and Therapeutics provides a forum for clinicians, pharmacists and pharmacologists to explore and report on issues of common interest. Reports and commentaries on current issues in medical and pharmaceutical practice are encouraged. Papers on evidence-based clinical practice and multidisciplinary collaborative work are particularly welcome. Regular sections in the journal include: editorials, commentaries, reviews (including systematic overviews and meta-analyses), original research and reports, and book reviews. Its scope embraces all aspects of clinical drug development and therapeutics, including:
Rational therapeutics
Evidence-based practice
Safety, cost-effectiveness and clinical efficacy of drugs
Drug interactions
Clinical impact of drug formulations
Pharmacogenetics
Personalised, stratified and translational medicine
Clinical pharmacokinetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


