Davi Freitas Tenório, Leonardo Augusto Miana, João Guilherme Vidal Meyer, Eric Shih Katsuyama, Christian Ken Fukunaga, Aida Luiza Ribeiro Turquetto, Luiza Patrick Amato, Marcelo Biscegli Jatene, Fabio B Jatene
{"title":"Technical Performance Score: A Robust Predictor of Morbidity Following the Norwood Procedure at a Developing Country Institution.","authors":"Davi Freitas Tenório, Leonardo Augusto Miana, João Guilherme Vidal Meyer, Eric Shih Katsuyama, Christian Ken Fukunaga, Aida Luiza Ribeiro Turquetto, Luiza Patrick Amato, Marcelo Biscegli Jatene, Fabio B Jatene","doi":"10.21470/1678-9741-2024-0442","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The Norwood operation has transformed the approach to hypoplastic left heart syndrome and its variants. Given the complexity of this procedure, postoperative residual injuries are prevalent.</p><p><strong>Objective: </strong>To evaluate the impact of significant residual injuries on clinical outcomes and mortality in Norwood procedure patients at a high-volume tertiary center in a developing nation using the technical performance score (TPS).</p><p><strong>Methods: </strong>This single-center, retrospective study included patients who underwent the Norwood procedure between December 2018 and February 2023. Data on demographics, echocardiograms, complications, intensive care unit stay, and mortality were collected. Logistic regression and linear analyses assessed the impact of TPS on outcomes.</p><p><strong>Results: </strong>Of 69 patients, nine (13%) were excluded due to incomplete echocardiographic data, leaving 60 (87%) for TPS classification. Among them, 28 (47%) were male. TPS classification was as follows: 40 (66%) in class 1 (excellent), five (8.3%) in class 2 (adequate), and 15 (25%) in class 3 (inadequate), indicating significant residual lesions or need for reintervention. The 30-day mortality rate was 21.6%, increasing to 41.6% before the next stage. In TPS class 3, 30-day mortality was 33% vs. 17% in classes 1 and 2 (P = 0.27). Interstage mortality was 60% in class 3 compared to 35% in other groups (P = 0.13). Major complications were significantly higher in TPS class 3 (93% vs. 55.5%, P = 0.04).</p><p><strong>Conclusion: </strong>TPS effectively predicts major complications post-Norwood and serves as a valuable tool for improving patient outcomes.</p>","PeriodicalId":72457,"journal":{"name":"Brazilian journal of cardiovascular surgery","volume":"40 4","pages":"e20240442"},"PeriodicalIF":1.2000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12175616/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brazilian journal of cardiovascular surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21470/1678-9741-2024-0442","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The Norwood operation has transformed the approach to hypoplastic left heart syndrome and its variants. Given the complexity of this procedure, postoperative residual injuries are prevalent.
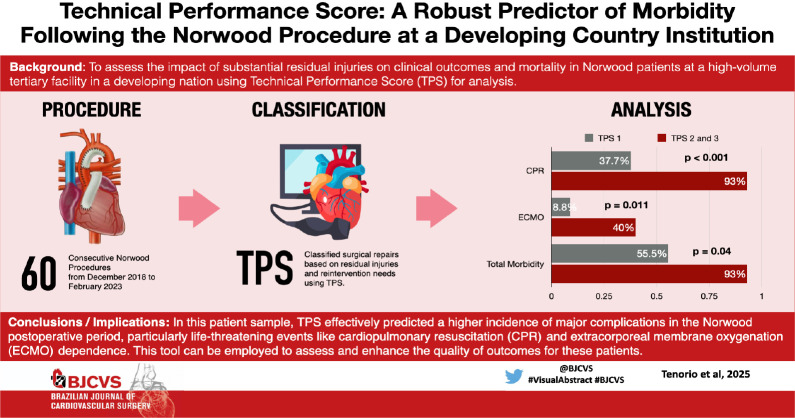
Objective: To evaluate the impact of significant residual injuries on clinical outcomes and mortality in Norwood procedure patients at a high-volume tertiary center in a developing nation using the technical performance score (TPS).
Methods: This single-center, retrospective study included patients who underwent the Norwood procedure between December 2018 and February 2023. Data on demographics, echocardiograms, complications, intensive care unit stay, and mortality were collected. Logistic regression and linear analyses assessed the impact of TPS on outcomes.
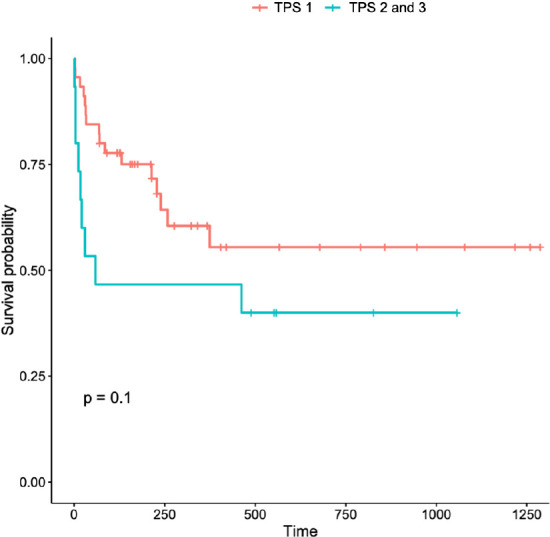
Results: Of 69 patients, nine (13%) were excluded due to incomplete echocardiographic data, leaving 60 (87%) for TPS classification. Among them, 28 (47%) were male. TPS classification was as follows: 40 (66%) in class 1 (excellent), five (8.3%) in class 2 (adequate), and 15 (25%) in class 3 (inadequate), indicating significant residual lesions or need for reintervention. The 30-day mortality rate was 21.6%, increasing to 41.6% before the next stage. In TPS class 3, 30-day mortality was 33% vs. 17% in classes 1 and 2 (P = 0.27). Interstage mortality was 60% in class 3 compared to 35% in other groups (P = 0.13). Major complications were significantly higher in TPS class 3 (93% vs. 55.5%, P = 0.04).
Conclusion: TPS effectively predicts major complications post-Norwood and serves as a valuable tool for improving patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


