Vikrant Khare, Travis Merritt, Natalia Zbib, Linnea Swanson, Maria Masotti, Robert J Fontana, Baljendra Kapoor, Hassan Anbari
{"title":"Right versus Middle Hepatic Vein access and One-Year TIPS Outcomes.","authors":"Vikrant Khare, Travis Merritt, Natalia Zbib, Linnea Swanson, Maria Masotti, Robert J Fontana, Baljendra Kapoor, Hassan Anbari","doi":"10.1186/s42155-025-00570-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study evaluates one-year clinical outcomes of transjugular intrahepatic portosystemic shunt (TIPS) placement using a middle hepatic vein (MHV) versus right hepatic vein (RHV) access. Primary end points were shunt patency and one-year survival. Secondary outcomes included incidence of de novo hepatic encephalopathy (HE) and recurrence of portal hypertension related complications such as ascites, hepatic hydrothorax, and gastrointestinal bleeding. While prior studies have examined portal vein target selection, the clinical relevance of hepatic vein choice remains understudied.</p><p><strong>Methods: </strong>A retrospective chart review of adult patients who underwent TIPS using a Viatorr stent graft between January 2014 and December 2022 was conducted. Patients were included if the procedure used either RHV or the MHV. Intracardiac echocardiography (ICE) was employed to select a direct path from hepatic to portal vein. Shunts were dilated to 8 or 10 mm to achieve a post-procedural portosystemic gradient (PSG) ≤ 12 mmHg or a 50% reduction from baseline. Clinical and imaging data was analyzed to assess outcomes, stratified by hepatic vein of access.</p><p><strong>Results: </strong>One-year survival (84% MHV vs 75% RHV, p = 0.2) and overall one-year patency rates (96% MHV vs 87% RHV, p = 0.5) were similar between the groups. However, MHV access significantly reduced de novo hepatic encephalopathy (30% MHV vs 62% RHV, p = 0.008) and moderate to severe cases (16% MHV vs 42% RHV, p = 0.017). Despite more frequent use of smaller diameter shunts (8 mm: 72% MHV vs 47% of RHV, p < 0.001), MHV access achieved similar post-TIPS portosystemic gradient reductions (Average Pre-TIPS gradient: 17 mmHg MHV & 17 mmHg RHV, p = 0.8; Average Post-TIPS gradient: 8 mmHg MHV & 7.5 mmHg RHV, p = 0.12). Hepatic vein choice did not affect outcomes for ascites, hydrothorax, or gastrointestinal bleeding.</p><p><strong>Conclusion: </strong>MHV and RHV access routes provided similar patency, survival, and TIPS indication outcomes, but MHV access had decreased incidence of hepatic encephalopathy and achieved similar portosystemic gradient reduction while using a smaller diameter shunt. MHV may be a preferred option for patients at higher risk of developing hepatic encephalopathy.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"8 1","pages":"54"},"PeriodicalIF":1.5000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12176723/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-025-00570-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study evaluates one-year clinical outcomes of transjugular intrahepatic portosystemic shunt (TIPS) placement using a middle hepatic vein (MHV) versus right hepatic vein (RHV) access. Primary end points were shunt patency and one-year survival. Secondary outcomes included incidence of de novo hepatic encephalopathy (HE) and recurrence of portal hypertension related complications such as ascites, hepatic hydrothorax, and gastrointestinal bleeding. While prior studies have examined portal vein target selection, the clinical relevance of hepatic vein choice remains understudied.
Methods: A retrospective chart review of adult patients who underwent TIPS using a Viatorr stent graft between January 2014 and December 2022 was conducted. Patients were included if the procedure used either RHV or the MHV. Intracardiac echocardiography (ICE) was employed to select a direct path from hepatic to portal vein. Shunts were dilated to 8 or 10 mm to achieve a post-procedural portosystemic gradient (PSG) ≤ 12 mmHg or a 50% reduction from baseline. Clinical and imaging data was analyzed to assess outcomes, stratified by hepatic vein of access.
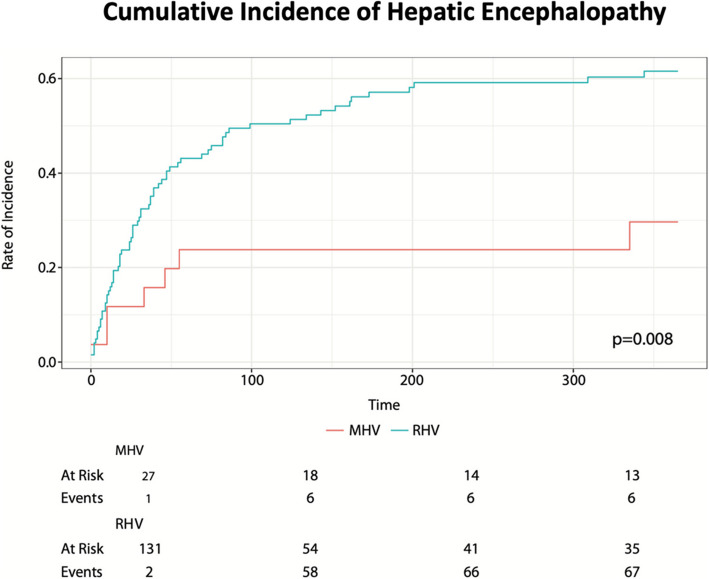
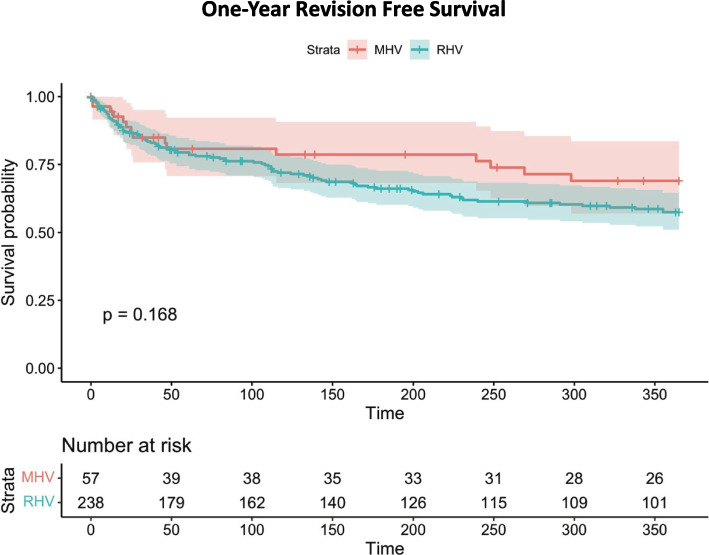
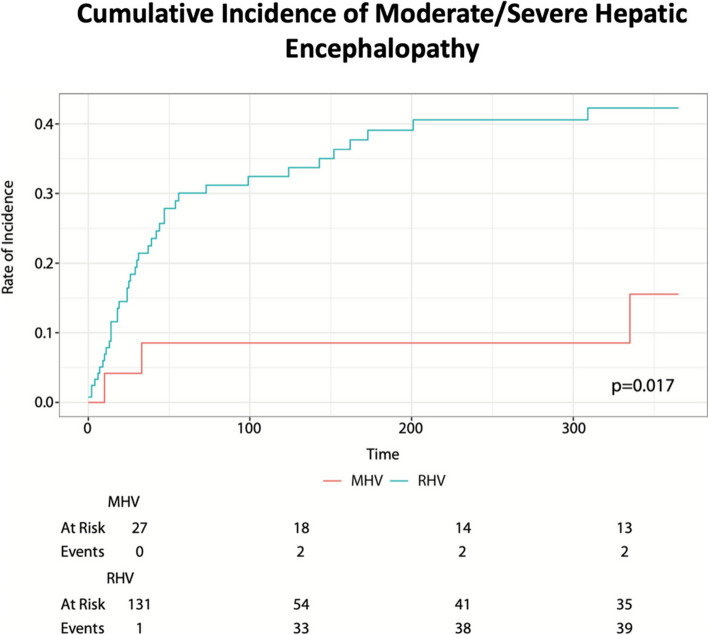
Results: One-year survival (84% MHV vs 75% RHV, p = 0.2) and overall one-year patency rates (96% MHV vs 87% RHV, p = 0.5) were similar between the groups. However, MHV access significantly reduced de novo hepatic encephalopathy (30% MHV vs 62% RHV, p = 0.008) and moderate to severe cases (16% MHV vs 42% RHV, p = 0.017). Despite more frequent use of smaller diameter shunts (8 mm: 72% MHV vs 47% of RHV, p < 0.001), MHV access achieved similar post-TIPS portosystemic gradient reductions (Average Pre-TIPS gradient: 17 mmHg MHV & 17 mmHg RHV, p = 0.8; Average Post-TIPS gradient: 8 mmHg MHV & 7.5 mmHg RHV, p = 0.12). Hepatic vein choice did not affect outcomes for ascites, hydrothorax, or gastrointestinal bleeding.
Conclusion: MHV and RHV access routes provided similar patency, survival, and TIPS indication outcomes, but MHV access had decreased incidence of hepatic encephalopathy and achieved similar portosystemic gradient reduction while using a smaller diameter shunt. MHV may be a preferred option for patients at higher risk of developing hepatic encephalopathy.
背景:本研究评估采用肝中静脉(MHV)与右肝静脉(RHV)通道经颈静脉肝内门静脉分流术(TIPS)放置一年的临床结果。主要终点为分流通畅和1年生存率。次要结局包括新发肝性脑病(HE)的发生率和门脉高压相关并发症的复发,如腹水、肝性胸水和胃肠道出血。虽然先前的研究已经检查了门静脉靶点的选择,但肝静脉选择的临床相关性仍未得到充分研究。方法:回顾性分析2014年1月至2022年12月期间使用Viatorr支架接受TIPS的成年患者的图表。如果手术使用RHV或MHV,则纳入患者。采用心内超声心动图(ICE)选择从肝静脉到门静脉的直接路径。将分流管扩张至8或10毫米,以达到术后门静脉系统梯度(PSG)≤12 mmHg或较基线降低50%。对临床和影像学资料进行分析以评估结果,并按肝静脉通路分层。结果:两组间一年生存率(84% MHV vs 75% RHV, p = 0.2)和总一年通畅率(96% MHV vs 87% RHV, p = 0.5)相似。然而,MHV治疗显著减少了新发肝性脑病(30% MHV vs 62% RHV, p = 0.008)和中至重度病例(16% MHV vs 42% RHV, p = 0.017)。尽管更频繁地使用较小直径的分流器(8mm: 72% MHV vs 47% RHV), p结论:MHV和RHV通路提供相似的通畅、生存和TIPS适应症结果,但MHV通路在使用较小直径分流器时降低了肝性脑病的发病率,并实现了相似的门静脉系统梯度降低。MHV可能是患肝性脑病风险较高的患者的首选。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


