The characteristics of HER2-positive microinvasive breast cancer and the necessity of systemic adjuvant therapy in these patients: a multicenter real-world study.
Bo Lan, Dan Lv, Changyuan Guo, Zitong Feng, Ying Fan, Tao Sun, Jiayi Huang, Xiaoying Sun, Fei Ma, Binghe Xu
{"title":"The characteristics of HER2-positive microinvasive breast cancer and the necessity of systemic adjuvant therapy in these patients: a multicenter real-world study.","authors":"Bo Lan, Dan Lv, Changyuan Guo, Zitong Feng, Ying Fan, Tao Sun, Jiayi Huang, Xiaoying Sun, Fei Ma, Binghe Xu","doi":"10.1177/17588359251345716","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is currently a lack of sufficient evidence on the prognosis of human epidermal factor receptor 2 (HER2)-positive microinvasive breast cancer (MIBC) and whether chemotherapy (CT) and targeted therapy can bring benefits.</p><p><strong>Objectives: </strong>To explore the prognosis and treatment of HER2-positive MIBC.</p><p><strong>Design: </strong>A retrospective multicenter study.</p><p><strong>Methods: </strong>In this multicenter real-world study, we consecutively enrolled patients who received local management and were diagnosed with lymph node-negative HER2-positive MIBC from January 2010 to December 2020.</p><p><strong>Results: </strong>A total of 163 patients were included. Thirty-nine patients (23.9%) received adjuvant CT, of which 12 patients (7.4%) received CT combined with trastuzumab. One patient received trastuzumab therapy alone. In total, nine patients (5.5%) experienced recurrence, and the 3-year disease-free survival (DFS) rate and 5-year DFS rate were both 95.1%. Kaplan-Meier analysis showed that patients aged ⩽40 had worse outcomes than those aged >40 (3-year DFS rate 81.8% vs 96.1%, <i>p</i> = 0.046). Using propensity score matching, we matched patients who received trastuzumab or CT ± trastuzumab with those who did not receive treatment based on age, tumor size, estrogen receptor status, and number of infiltration lesions. Patients who received targeted therapy or CT ± targeted therapy did not achieve further improvement in 3-year DFS rate (95.0% vs 95.0%, <i>p</i> = 0.630).</p><p><strong>Conclusion: </strong>HER2-positive MIBC has relatively good prognosis, and age ⩽40 years might be a poor prognostic factor. CT or targeted therapy seemed to bring little benefit for MIBC. Further prospective studies are needed to assess potential benefits of management for MIBC patients under the age of 40 years in the future.</p>","PeriodicalId":23053,"journal":{"name":"Therapeutic Advances in Medical Oncology","volume":"17 ","pages":"17588359251345716"},"PeriodicalIF":4.2000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12174808/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Medical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17588359251345716","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is currently a lack of sufficient evidence on the prognosis of human epidermal factor receptor 2 (HER2)-positive microinvasive breast cancer (MIBC) and whether chemotherapy (CT) and targeted therapy can bring benefits.
Objectives: To explore the prognosis and treatment of HER2-positive MIBC.
Design: A retrospective multicenter study.
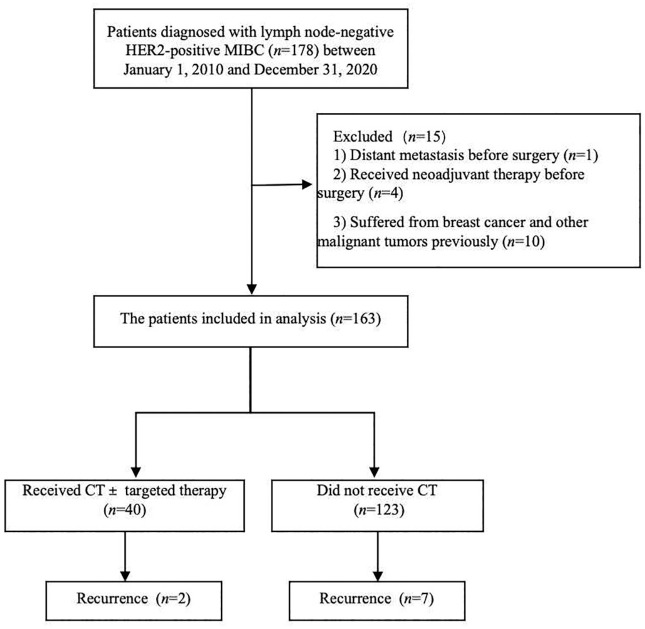
Methods: In this multicenter real-world study, we consecutively enrolled patients who received local management and were diagnosed with lymph node-negative HER2-positive MIBC from January 2010 to December 2020.
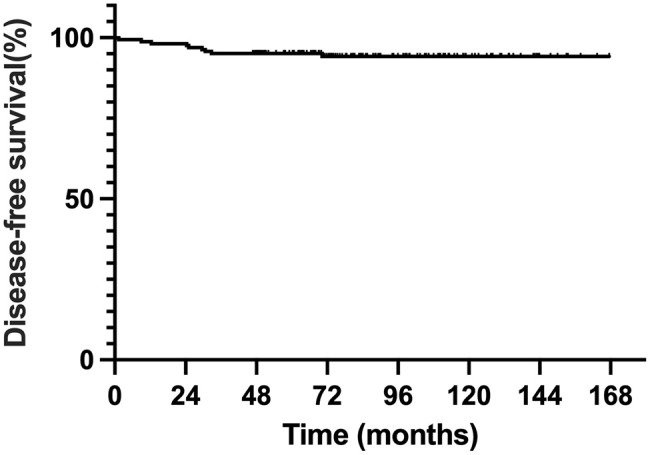
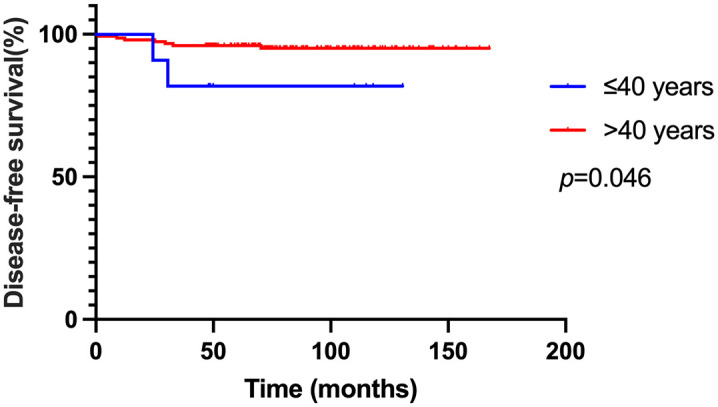
Results: A total of 163 patients were included. Thirty-nine patients (23.9%) received adjuvant CT, of which 12 patients (7.4%) received CT combined with trastuzumab. One patient received trastuzumab therapy alone. In total, nine patients (5.5%) experienced recurrence, and the 3-year disease-free survival (DFS) rate and 5-year DFS rate were both 95.1%. Kaplan-Meier analysis showed that patients aged ⩽40 had worse outcomes than those aged >40 (3-year DFS rate 81.8% vs 96.1%, p = 0.046). Using propensity score matching, we matched patients who received trastuzumab or CT ± trastuzumab with those who did not receive treatment based on age, tumor size, estrogen receptor status, and number of infiltration lesions. Patients who received targeted therapy or CT ± targeted therapy did not achieve further improvement in 3-year DFS rate (95.0% vs 95.0%, p = 0.630).
Conclusion: HER2-positive MIBC has relatively good prognosis, and age ⩽40 years might be a poor prognostic factor. CT or targeted therapy seemed to bring little benefit for MIBC. Further prospective studies are needed to assess potential benefits of management for MIBC patients under the age of 40 years in the future.
背景:目前关于人表皮因子受体2 (HER2)阳性的微创乳腺癌(MIBC)的预后以及化疗(CT)和靶向治疗是否能带来益处的证据还不够充分。目的:探讨her2阳性MIBC的预后及治疗方法。设计:回顾性多中心研究。方法:在这项多中心现实世界研究中,我们从2010年1月至2020年12月连续招募了接受局部治疗并被诊断为淋巴结阴性her2阳性MIBC的患者。结果:共纳入163例患者。39例(23.9%)患者接受了辅助CT,其中12例(7.4%)患者接受了CT联合曲妥珠单抗。1例患者单独接受曲妥珠单抗治疗。9例(5.5%)复发,3年无病生存率(DFS)和5年DFS均为95.1%。Kaplan-Meier分析显示,年龄≥40岁的患者预后较年龄≥40岁的患者差(3年DFS率81.8% vs 96.1%, p = 0.046)。使用倾向评分匹配,我们将接受曲妥珠单抗或CT±曲妥珠单抗治疗的患者与未接受治疗的患者根据年龄、肿瘤大小、雌激素受体状态和浸润病变数量进行匹配。接受靶向治疗或CT±靶向治疗的患者3年DFS率没有进一步改善(95.0% vs 95.0%, p = 0.630)。结论:her2阳性的MIBC预后较好,年龄≥40岁可能是预后不良的因素。CT或靶向治疗似乎对MIBC没有什么好处。未来需要进一步的前瞻性研究来评估治疗40岁以下MIBC患者的潜在益处。
期刊介绍:
Therapeutic Advances in Medical Oncology is an open access, peer-reviewed journal delivering the highest quality articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of cancer. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in medical oncology, providing a forum in print and online for publishing the highest quality articles in this area. This journal is a member of the Committee on Publication Ethics (COPE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


