Nicolás Lundahl Ciano-Petersen, Macarena Villagrán-García, Sergio Muñiz-Castrillo, Antonio Farina, Alberto Vogrig, David Goncalves, Fabien Nicole, Véronique Rogemond, Geraldine Picard, Mélodie Aubart, Dimitri Psimaras, Begoña Oliver, Pedro J Serrano-Castro, Bastien Joubert, Jerome Honnorat
{"title":"Relapses in Anti-NMDAR Encephalitis: Clinical Characterization and Predictive Features.","authors":"Nicolás Lundahl Ciano-Petersen, Macarena Villagrán-García, Sergio Muñiz-Castrillo, Antonio Farina, Alberto Vogrig, David Goncalves, Fabien Nicole, Véronique Rogemond, Geraldine Picard, Mélodie Aubart, Dimitri Psimaras, Begoña Oliver, Pedro J Serrano-Castro, Bastien Joubert, Jerome Honnorat","doi":"10.1212/NXI.0000000000200421","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>During the recovery phase of anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis, up to 25% of relapses have been reported. Herein, we aimed to clinically characterize these relapses, analyze potential clinical predictors during the first episode, and evaluate the impact of immunotherapy in their occurrence.</p><p><strong>Methods: </strong>This was a retrospective observational study of patients diagnosed with anti-NMDAR encephalitis relapses between January 2007 and June 2022 at the French Reference Center for Paraneoplastic Neurological Syndromes and Autoimmune Encephalitis with a follow-up longer than 1 year.</p><p><strong>Results: </strong>Among 507 patients, 49 (9%) presented relapses after a median time of 720 days (range 149-8,280) and a median follow-up of 1752 days (range 390-9,229 days, interquartile range 1760 days). A total of 36 patients (73%) experienced 1 relapse, 9 (18%) had 2, and 4 (8%) had 3 relapses. Most patients presented an isolated core symptom (25/45, 55%). Relapses were less severe than the first episode, as reflected by a lower maximal modified Rankin Scale (median 5, range 3-5, vs median 3, range 0-6; <i>p</i> = 0.0001). At the first episode, patients experiencing relapses had shorter intensive care unit stays (22 days; vs 39 days; <i>p</i> = 0.04). In addition, presenting CSF pleocytosis >20 white blood cell decreased the risk of relapse by 71% (HR 0.29; CI 0.13-0.66; <i>p</i> = 0.003), and having a paraneoplastic etiology decreased the risk by 68% (HR 0.32; CI 0.12-0.87; <i>p</i> = 0.02). Moreover, during the first episode, they were treated less frequently with first-line (39/49, 79%, vs 190/197, 96%; <i>p</i> = 0.0001) and second-line immunotherapies (20/49, 40%, vs 142/197, 72%; <i>p</i> = 0.0001) and more frequently with delay >30 days (20/38, 52%, vs 58/185, 31%; <i>p</i> = 0.01) and >60 days (10/20, 50%, vs 39/138, 28%; <i>p</i> = 0.04), respectively. In addition, administering rituximab during the first episode with a delay <60 days decreased the risk of relapse by 60% (HR 0.40; CI 0.19-0.84; <i>p</i> = 0.01).</p><p><strong>Discussion: </strong>Relapses of anti-NMDAR encephalitis are uncommon, mostly monosymptomatic, and less severe than the first episode. At onset, presenting CSF pleocytosis or an underlying tumor decreases the risk of relapses. In addition, the early administration of first-line and second-line immunotherapies, particularly rituximab, could protect against further relapses.</p>","PeriodicalId":19472,"journal":{"name":"Neurology® Neuroimmunology & Neuroinflammation","volume":"12 4","pages":"e200421"},"PeriodicalIF":7.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185219/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology® Neuroimmunology & Neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200421","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: During the recovery phase of anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis, up to 25% of relapses have been reported. Herein, we aimed to clinically characterize these relapses, analyze potential clinical predictors during the first episode, and evaluate the impact of immunotherapy in their occurrence.
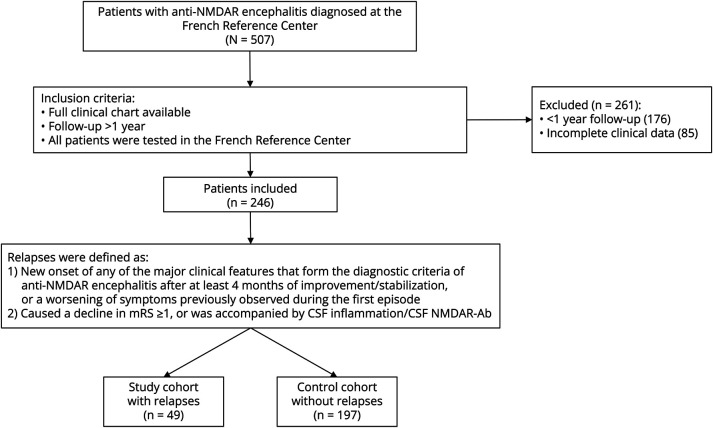
Methods: This was a retrospective observational study of patients diagnosed with anti-NMDAR encephalitis relapses between January 2007 and June 2022 at the French Reference Center for Paraneoplastic Neurological Syndromes and Autoimmune Encephalitis with a follow-up longer than 1 year.
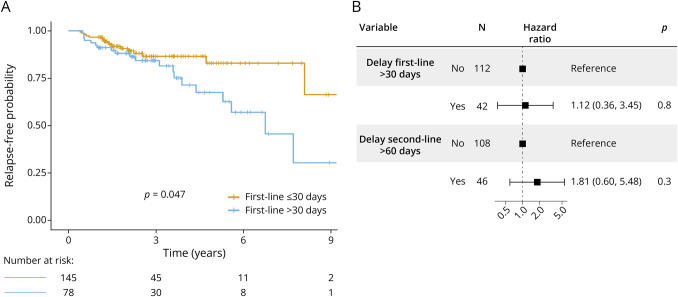
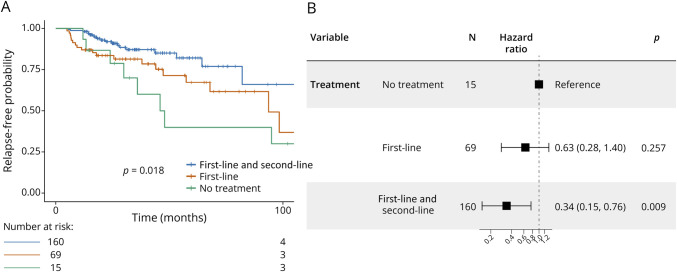
Results: Among 507 patients, 49 (9%) presented relapses after a median time of 720 days (range 149-8,280) and a median follow-up of 1752 days (range 390-9,229 days, interquartile range 1760 days). A total of 36 patients (73%) experienced 1 relapse, 9 (18%) had 2, and 4 (8%) had 3 relapses. Most patients presented an isolated core symptom (25/45, 55%). Relapses were less severe than the first episode, as reflected by a lower maximal modified Rankin Scale (median 5, range 3-5, vs median 3, range 0-6; p = 0.0001). At the first episode, patients experiencing relapses had shorter intensive care unit stays (22 days; vs 39 days; p = 0.04). In addition, presenting CSF pleocytosis >20 white blood cell decreased the risk of relapse by 71% (HR 0.29; CI 0.13-0.66; p = 0.003), and having a paraneoplastic etiology decreased the risk by 68% (HR 0.32; CI 0.12-0.87; p = 0.02). Moreover, during the first episode, they were treated less frequently with first-line (39/49, 79%, vs 190/197, 96%; p = 0.0001) and second-line immunotherapies (20/49, 40%, vs 142/197, 72%; p = 0.0001) and more frequently with delay >30 days (20/38, 52%, vs 58/185, 31%; p = 0.01) and >60 days (10/20, 50%, vs 39/138, 28%; p = 0.04), respectively. In addition, administering rituximab during the first episode with a delay <60 days decreased the risk of relapse by 60% (HR 0.40; CI 0.19-0.84; p = 0.01).
Discussion: Relapses of anti-NMDAR encephalitis are uncommon, mostly monosymptomatic, and less severe than the first episode. At onset, presenting CSF pleocytosis or an underlying tumor decreases the risk of relapses. In addition, the early administration of first-line and second-line immunotherapies, particularly rituximab, could protect against further relapses.
期刊介绍:
Neurology Neuroimmunology & Neuroinflammation is an official journal of the American Academy of Neurology. Neurology: Neuroimmunology & Neuroinflammation will be the premier peer-reviewed journal in neuroimmunology and neuroinflammation. This journal publishes rigorously peer-reviewed open-access reports of original research and in-depth reviews of topics in neuroimmunology & neuroinflammation, affecting the full range of neurologic diseases including (but not limited to) Alzheimer's disease, Parkinson's disease, ALS, tauopathy, and stroke; multiple sclerosis and NMO; inflammatory peripheral nerve and muscle disease, Guillain-Barré and myasthenia gravis; nervous system infection; paraneoplastic syndromes, noninfectious encephalitides and other antibody-mediated disorders; and psychiatric and neurodevelopmental disorders. Clinical trials, instructive case reports, and small case series will also be featured.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


