Association between ultrasound-based biliary and parenchymal intrahepatic mass-forming cholangiocarcinoma subtypes and clinicopathological features and survival.
IF 4.5 2区 医学Q1 RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
{"title":"Association between ultrasound-based biliary and parenchymal intrahepatic mass-forming cholangiocarcinoma subtypes and clinicopathological features and survival.","authors":"Cong-Jian Wen, Hui Liu, Li-Ping Sun, Chong-Ke Zhao, Hao-Hao Yin, Li-Fan Wang, Ming-Rui Zhu, Yi-Kang Sun, Ya-Qin Zhang, Zi-Tong Chen, Xi Wang, Han-Sheng Xia, Hong Han, Hui-Xiong Xu, Bo-Yang Zhou","doi":"10.1186/s13244-025-02019-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Mass-forming intrahepatic cholangiocarcinomas (MF-ICCs) can be classified into ductal and parenchymal types using magnetic resonance imaging (MRI). We aimed to subclassify MF-ICC into biliary and parenchymal types based on ultrasound (US) findings and to investigate the differences in their contrast-enhanced ultrasound (CEUS) patterns, clinicopathologic features, and prognosis.</p><p><strong>Methods: </strong>In this study, 141 patients who underwent US with pathologically proven MF-ICC from two hospitals were retrospectively enrolled. MF-ICCs were divided into biliary (bMF-ICCs) and parenchymal MF-ICC (pMF-ICCs) based on the signs of bile duct dilation in US images. Clinicopathological, imaging, and short-term survival data were collected from medical records and compared.</p><p><strong>Results: </strong>Among 141 patients (61.96 ± 10.15 years, 83 men), bMF-ICCs (33/141, 23.4%) showed significantly more CEA ≥ 5 µg/L (42.4% vs 20.2%, p = 0.01), microvascular invasion (54.5% vs 10.2%, p < 0.001), lymph node metastasis (48.5% vs 5.6%, p < 0.001), bile duct invasion (48.5% vs 5.6%, p < 0.001), and high Ki-67 expression (63.6% vs 38.9%, p = 0.01) than pMF-ICCs. Pathologically, bMF-ICCs were more inclined toward the large duct type (78.1% vs 11.7%, p < 0.001). In addition, the bMF-ICCs were usually located in the left lobe of the liver (63.6% vs 41.7%, p = 0.03). pMF-ICCs showed better overall survival than bMF-ICCs (p = 0.04).</p><p><strong>Conclusions: </strong>Subclassification of MF-ICCs into biliary and parenchymal types based on US is useful for discriminating clinicopathological characteristics.</p><p><strong>Critical relevance statement: </strong>The subclassification of mass-forming intrahepatic cholangiocarcinoma (MF-ICC) into biliary (bMF-ICC) and parenchymal (pMF-ICC) subtypes using ultrasound can provide clinicopathological and prognostic information before surgery.</p><p><strong>Key points: </strong>We subclassified mass-forming intrahepatic cholangiocarcinomas into biliary and parenchymal types using ultrasound. Biliary and parenchymal types have different clinicopathological features and postsurgical outcomes. Biliary type above and below 50 mm exhibits different unfavorable clinicopathological characteristics. Our classification has certain similarities with MRI classification in clinicopathological characteristics.</p>","PeriodicalId":13639,"journal":{"name":"Insights into Imaging","volume":"16 1","pages":"130"},"PeriodicalIF":4.5000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179021/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Insights into Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13244-025-02019-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Mass-forming intrahepatic cholangiocarcinomas (MF-ICCs) can be classified into ductal and parenchymal types using magnetic resonance imaging (MRI). We aimed to subclassify MF-ICC into biliary and parenchymal types based on ultrasound (US) findings and to investigate the differences in their contrast-enhanced ultrasound (CEUS) patterns, clinicopathologic features, and prognosis.
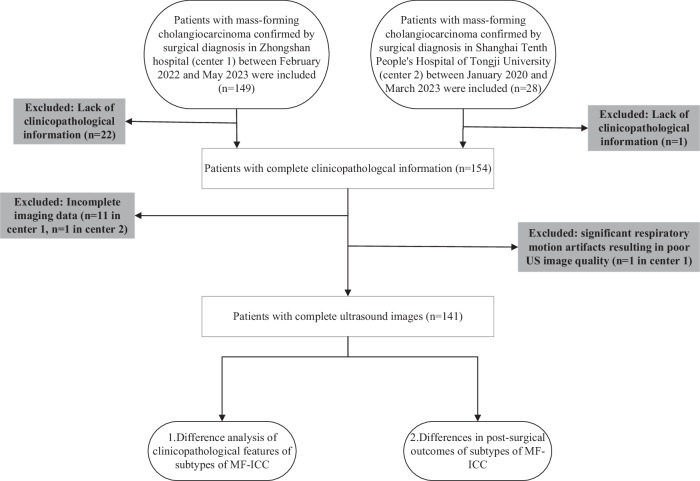
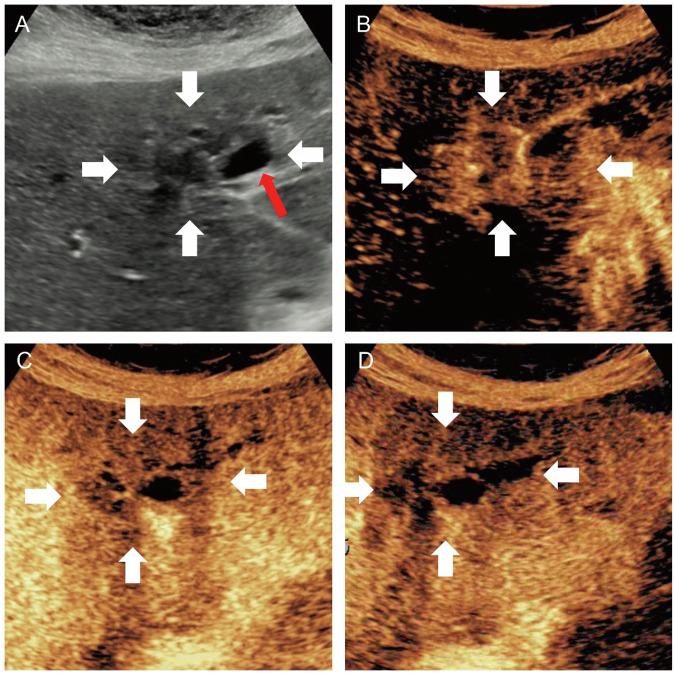
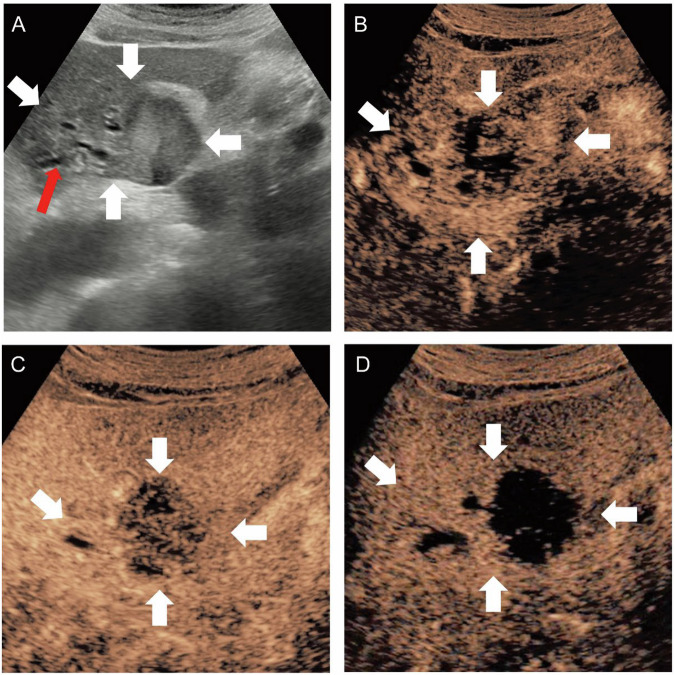
Methods: In this study, 141 patients who underwent US with pathologically proven MF-ICC from two hospitals were retrospectively enrolled. MF-ICCs were divided into biliary (bMF-ICCs) and parenchymal MF-ICC (pMF-ICCs) based on the signs of bile duct dilation in US images. Clinicopathological, imaging, and short-term survival data were collected from medical records and compared.
Results: Among 141 patients (61.96 ± 10.15 years, 83 men), bMF-ICCs (33/141, 23.4%) showed significantly more CEA ≥ 5 µg/L (42.4% vs 20.2%, p = 0.01), microvascular invasion (54.5% vs 10.2%, p < 0.001), lymph node metastasis (48.5% vs 5.6%, p < 0.001), bile duct invasion (48.5% vs 5.6%, p < 0.001), and high Ki-67 expression (63.6% vs 38.9%, p = 0.01) than pMF-ICCs. Pathologically, bMF-ICCs were more inclined toward the large duct type (78.1% vs 11.7%, p < 0.001). In addition, the bMF-ICCs were usually located in the left lobe of the liver (63.6% vs 41.7%, p = 0.03). pMF-ICCs showed better overall survival than bMF-ICCs (p = 0.04).
Conclusions: Subclassification of MF-ICCs into biliary and parenchymal types based on US is useful for discriminating clinicopathological characteristics.
Critical relevance statement: The subclassification of mass-forming intrahepatic cholangiocarcinoma (MF-ICC) into biliary (bMF-ICC) and parenchymal (pMF-ICC) subtypes using ultrasound can provide clinicopathological and prognostic information before surgery.
Key points: We subclassified mass-forming intrahepatic cholangiocarcinomas into biliary and parenchymal types using ultrasound. Biliary and parenchymal types have different clinicopathological features and postsurgical outcomes. Biliary type above and below 50 mm exhibits different unfavorable clinicopathological characteristics. Our classification has certain similarities with MRI classification in clinicopathological characteristics.
期刊介绍:
Insights into Imaging (I³) is a peer-reviewed open access journal published under the brand SpringerOpen. All content published in the journal is freely available online to anyone, anywhere!
I³ continuously updates scientific knowledge and progress in best-practice standards in radiology through the publication of original articles and state-of-the-art reviews and opinions, along with recommendations and statements from the leading radiological societies in Europe.
Founded by the European Society of Radiology (ESR), I³ creates a platform for educational material, guidelines and recommendations, and a forum for topics of controversy.
A balanced combination of review articles, original papers, short communications from European radiological congresses and information on society matters makes I³ an indispensable source for current information in this field.
I³ is owned by the ESR, however authors retain copyright to their article according to the Creative Commons Attribution License (see Copyright and License Agreement). All articles can be read, redistributed and reused for free, as long as the author of the original work is cited properly.
The open access fees (article-processing charges) for this journal are kindly sponsored by ESR for all Members.
The journal went open access in 2012, which means that all articles published since then are freely available online.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


