{"title":"A qualitative study on the barriers to tuberculosis treatment adherence using digital adherence technologies (DATs).","authors":"Madhuvarshne Sivashanmugam, Rajalakshmi Mahendran","doi":"10.25259/IJMR_1644_2024","DOIUrl":null,"url":null,"abstract":"<p><p>Background & objectives In order to meet the ambitious aim set by the Government of India as well as the sustainable development goals (SDG) target for eliminating tuberculosis in 2030, it is important for the healthcare providers to follow and support the patients throughout the treatment for its successful completion. For monitoring the tuberculosis treatment compliance, Digital Adherence Technologies (DATs) play a major role. DATs are digital tools that use mobile phone, computer, or sensor technologies to support the capture of detailed, daily, patient-specific adherence information. DATs provide opportunities for a more patient-centred care model and also help healthcare workers while treating tuberculosis (TB) patients when compared to traditional directly observed therapy. Hence, in this study explored the acceptance and barriers to the use of DATs for monitoring compliance with TB treatment and its possible solutions. Methods A community-based qualitative study was done in two PHCs in Puducherry, India among TB patients who completed treatment, healthcare providers such as tuberculosis health visitors, staff nurses, and respective medical officers. Thirty participants were interviewed using purposive sampling to explore TB treatment outcomes over two months (Oct-Nov 2023). In-depth interviews were conducted with the help of a separate interview guide consisting of broad, open-ended questions with two primary stimulus questions based on the acceptance and barriers for use of DATs for capturing adherence to TB treatment. The possible solutions for the barriers to the use of DATs were also explored by the healthcare providers. Manual content analysis was done for the qualitative data. Results Benefits of the use of DATs included saving time, identification of loss to follow up patients, information on NIKSHAY, and other direct benefit transfers. Barriers include financial constraints, level of education, family issues, and difficulty in the use of gadgets (tab). Some of the solutions to the barriers were cooperation from family members, distribution of mobile phones, appointment of ASHA workers, and linking of NIKSHAY IDs with Aadhaar card numbers to avoid duplication. Interpretation & Conclusions Identification of barriers and potential solutions in DATs can help in the successful monitoring and completion of tuberculosis treatment which are crucial towards achieving the tuberculosis elimination goal set by the Government of India as well as the SDG target for elimination by 2030.</p>","PeriodicalId":13349,"journal":{"name":"Indian Journal of Medical Research","volume":"161 4","pages":"354-361"},"PeriodicalIF":2.5000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178189/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Medical Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.25259/IJMR_1644_2024","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
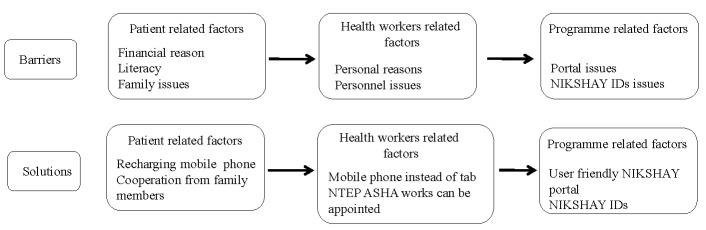
Background & objectives In order to meet the ambitious aim set by the Government of India as well as the sustainable development goals (SDG) target for eliminating tuberculosis in 2030, it is important for the healthcare providers to follow and support the patients throughout the treatment for its successful completion. For monitoring the tuberculosis treatment compliance, Digital Adherence Technologies (DATs) play a major role. DATs are digital tools that use mobile phone, computer, or sensor technologies to support the capture of detailed, daily, patient-specific adherence information. DATs provide opportunities for a more patient-centred care model and also help healthcare workers while treating tuberculosis (TB) patients when compared to traditional directly observed therapy. Hence, in this study explored the acceptance and barriers to the use of DATs for monitoring compliance with TB treatment and its possible solutions. Methods A community-based qualitative study was done in two PHCs in Puducherry, India among TB patients who completed treatment, healthcare providers such as tuberculosis health visitors, staff nurses, and respective medical officers. Thirty participants were interviewed using purposive sampling to explore TB treatment outcomes over two months (Oct-Nov 2023). In-depth interviews were conducted with the help of a separate interview guide consisting of broad, open-ended questions with two primary stimulus questions based on the acceptance and barriers for use of DATs for capturing adherence to TB treatment. The possible solutions for the barriers to the use of DATs were also explored by the healthcare providers. Manual content analysis was done for the qualitative data. Results Benefits of the use of DATs included saving time, identification of loss to follow up patients, information on NIKSHAY, and other direct benefit transfers. Barriers include financial constraints, level of education, family issues, and difficulty in the use of gadgets (tab). Some of the solutions to the barriers were cooperation from family members, distribution of mobile phones, appointment of ASHA workers, and linking of NIKSHAY IDs with Aadhaar card numbers to avoid duplication. Interpretation & Conclusions Identification of barriers and potential solutions in DATs can help in the successful monitoring and completion of tuberculosis treatment which are crucial towards achieving the tuberculosis elimination goal set by the Government of India as well as the SDG target for elimination by 2030.
期刊介绍:
The Indian Journal of Medical Research (IJMR) [ISSN 0971-5916] is one of the oldest medical Journals not only in India, but probably in Asia, as it started in the year 1913. The Journal was started as a quarterly (4 issues/year) in 1913 and made bimonthly (6 issues/year) in 1958. It became monthly (12 issues/year) in the year 1964.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


