Tao Huang, Lijuan Chen, Xiaoyi Liu, Ke Wang, Weiwei Shu, Lei Jiang, Linfu Bai, Wenhui Hu, Mengyi Ma, Jun Duan
{"title":"Association between early intubation and mortality in patients at high risk for noninvasive ventilation failure: a propensity-matched cohort study.","authors":"Tao Huang, Lijuan Chen, Xiaoyi Liu, Ke Wang, Weiwei Shu, Lei Jiang, Linfu Bai, Wenhui Hu, Mengyi Ma, Jun Duan","doi":"10.1177/17534666251347757","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Noninvasive ventilation (NIV) is frequently employed for acute hypoxemic respiratory failure, yet optimal intubation timing for high-risk NIV failure patients remains uncertain.</p><p><strong>Objectives: </strong>To investigate mortality outcomes associated with early versus late intubation in high-risk NIV failure patients.</p><p><strong>Design: </strong>Secondary analysis of a multicenter observational cohort study.</p><p><strong>Methods: </strong>Patients with high NIV failure risk (updated HACOR score ⩾11 after 1-2 h of NIV) were enrolled. We defined that intubation was needed in these high-risk patients. Intubation occurring within 12 h of NIV initiation was classified as early intubation, while intubation after 12 h was designated as late intubation. Primary outcomes were intensive care unit (ICU) and hospital mortality. In sensitivity analyses, patients who achieved NIV success were categorized into the late-intubation group. Due to baseline imbalances, propensity score matching was performed with covariate adjustment.</p><p><strong>Results: </strong>Among the study population, 171 patients underwent early intubation and 222 underwent late intubation. Despite greater baseline severity in the early intubation group, ICU mortality (36% vs 58%, <i>p</i> < 0.001) and hospital mortality (38% vs 58%, <i>p</i> < 0.001) were significantly lower compared to the late-intubation group. In sensitivity analyses, 190 patients with NIV success were included in the late-intubation group, further accentuating the severity disparity between groups. After propensity matching (220 patients: 110 per group), most of the baseline characteristics were comparable. The early intubation group had a 100% intubation rate versus 71% in the late-intubation group, with the latter exhibiting higher mortality (ICU: 46% vs 32%, <i>p</i> = 0.052; hospital: 50% vs 34%, <i>p</i> = 0.020).</p><p><strong>Conclusion: </strong>In patients at high risk for NIV failure, early intubation is associated with reduced mortality.</p>","PeriodicalId":22884,"journal":{"name":"Therapeutic Advances in Respiratory Disease","volume":"19 ","pages":"17534666251347757"},"PeriodicalIF":3.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12177261/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17534666251347757","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/18 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Noninvasive ventilation (NIV) is frequently employed for acute hypoxemic respiratory failure, yet optimal intubation timing for high-risk NIV failure patients remains uncertain.
Objectives: To investigate mortality outcomes associated with early versus late intubation in high-risk NIV failure patients.
Design: Secondary analysis of a multicenter observational cohort study.
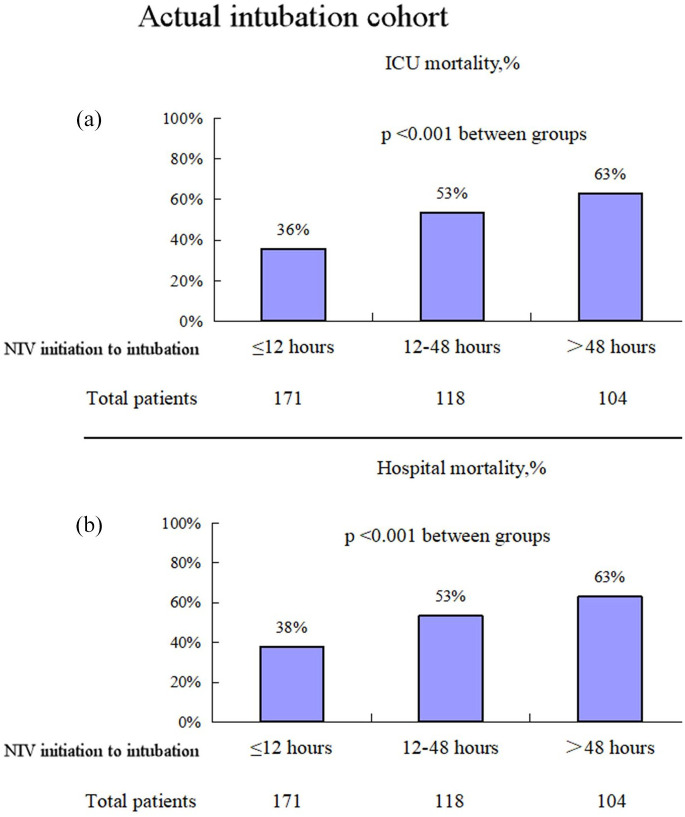
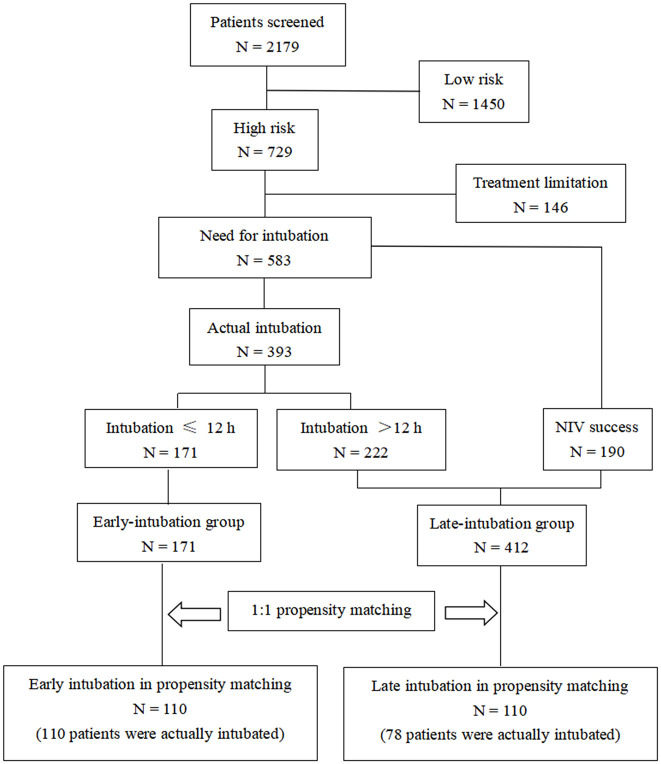
Methods: Patients with high NIV failure risk (updated HACOR score ⩾11 after 1-2 h of NIV) were enrolled. We defined that intubation was needed in these high-risk patients. Intubation occurring within 12 h of NIV initiation was classified as early intubation, while intubation after 12 h was designated as late intubation. Primary outcomes were intensive care unit (ICU) and hospital mortality. In sensitivity analyses, patients who achieved NIV success were categorized into the late-intubation group. Due to baseline imbalances, propensity score matching was performed with covariate adjustment.
Results: Among the study population, 171 patients underwent early intubation and 222 underwent late intubation. Despite greater baseline severity in the early intubation group, ICU mortality (36% vs 58%, p < 0.001) and hospital mortality (38% vs 58%, p < 0.001) were significantly lower compared to the late-intubation group. In sensitivity analyses, 190 patients with NIV success were included in the late-intubation group, further accentuating the severity disparity between groups. After propensity matching (220 patients: 110 per group), most of the baseline characteristics were comparable. The early intubation group had a 100% intubation rate versus 71% in the late-intubation group, with the latter exhibiting higher mortality (ICU: 46% vs 32%, p = 0.052; hospital: 50% vs 34%, p = 0.020).
Conclusion: In patients at high risk for NIV failure, early intubation is associated with reduced mortality.
背景:无创通气(NIV)常用于急性低氧血症性呼吸衰竭,但对高危无创通气失败患者的最佳插管时间仍不确定。目的:探讨高危无创通气失败患者早期与晚期插管相关的死亡率。设计:多中心观察队列研究的二次分析。方法:招募NIV失败风险高的患者(在NIV 1-2小时后更新HACOR评分大于或等于11)。我们确定这些高危患者需要插管。在NIV启动后12小时内插管被归类为早期插管,12小时后插管被归类为晚期插管。主要结局是重症监护病房(ICU)和住院死亡率。在敏感性分析中,获得NIV成功的患者被归类为晚期插管组。由于基线不平衡,倾向评分匹配进行协变量调整。结果:在研究人群中,早期插管171例,晚期插管222例。尽管早期插管组的基线严重程度更高,但ICU死亡率(36% vs 58%, p p p = 0.052;医院:50% vs 34%, p = 0.020)。结论:在NIV失效的高危患者中,早期插管可降低死亡率。
期刊介绍:
Therapeutic Advances in Respiratory Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of respiratory disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


