Timothy P Webber, Benjamin J Young, Marianne J Chapman, Mark E Finnis
{"title":"Complications of induced hypertension for delayed cerebral ischaemia secondary to aneurysmal subarachnoid haemorrhage.","authors":"Timothy P Webber, Benjamin J Young, Marianne J Chapman, Mark E Finnis","doi":"10.1177/0310057X251330315","DOIUrl":null,"url":null,"abstract":"<p><p>The study objective was to determine the incidence of complications from induced hypertension used to treat delayed cerebral ischaemia (DCI) complicating aneurysmal subarachnoid haemorrhage (aSAH). Induced hypertension (IH) was defined as the use of vasopressors to achieve a supraphysiological systolic blood pressure target. A single-centre retrospective, observational cohort study was undertaken at the Royal Adelaide Hospital intensive care unit. Data are presented as predominantly median (interquartile range (IQR)). All patients admitted with a diagnosis of aSAH between 1 April 2020 and 1 April 2022 were included and analysed according to whether they did or did not receive vasopressors for IH. A total of 109 patients were included, of which 29 (27%) received vasopressors for IH (median age 58 (IQR 52-65) years, 65% female) and 80 did not receive IH (median age 55 (IQR 49-71) years, 62% female). Clinical DCI or radiological evidence of vasospasm were present in all patients given IH and in 16% of non-IH patients. Patients in the IH group had more ischaemic electrocardiogram (ECG) changes (17.2% <i>vs</i> 2.5%, <i>P</i> = 0.01), urine output (4807 (IQR 3186-5720) ml/day <i>vs</i> 2125 (IQR 1650-2760) ml/day, <i>P</i> < 0.001), fluid administration (4895 (IQR 3555-5999) ml/day <i>vs</i> 2704 (IQR 2300-3403) ml/day, <i>P</i> < 0.001) and intravenous potassium replacement (13 (IQR 5-24) mmol/day <i>vs</i> 5 (IQR 0-13) mmol/day, <i>P</i> = 0.001) than those in the non-IH group. IH was also associated with a greater incidence of hyponatraemia (58% <i>vs</i> 34%, <i>P</i> = 0.02). IH was not associated with arrhythmias or rebleeding. Mortality rates were 17% <i>vs</i> 20% (<i>P</i> > 0.9) in the IH and non-IH groups respectively. In conclusion, IH for the treatment of DCI following aSAH was associated with an increased rate of ischaemic ECG changes, increased urine output and hyponatraemia. However, in the IH group there was no increased rate of rebleeding, and 48% of the IH patients had an improvement in their neurological function following commencement of treatment.</p>","PeriodicalId":7746,"journal":{"name":"Anaesthesia and Intensive Care","volume":" ","pages":"315-323"},"PeriodicalIF":1.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12420932/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia and Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/0310057X251330315","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
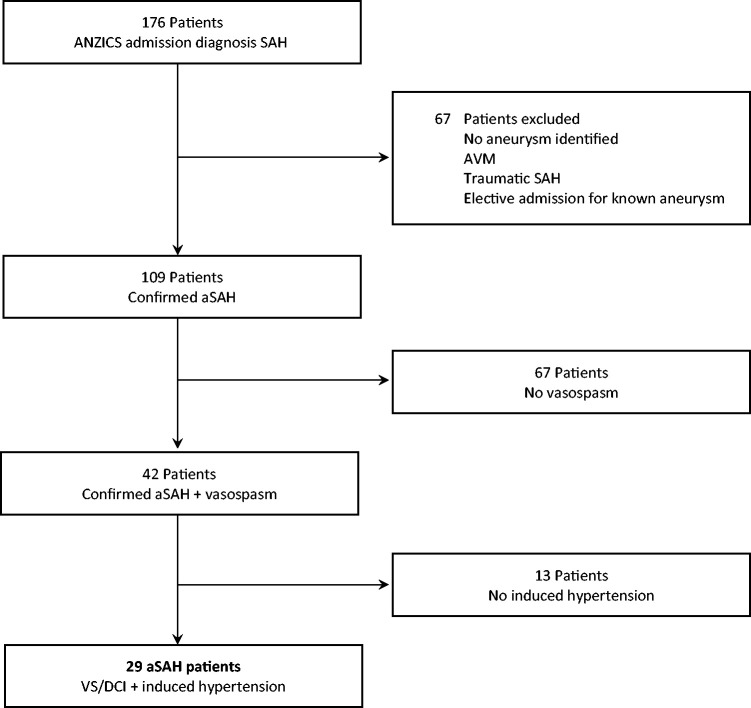
The study objective was to determine the incidence of complications from induced hypertension used to treat delayed cerebral ischaemia (DCI) complicating aneurysmal subarachnoid haemorrhage (aSAH). Induced hypertension (IH) was defined as the use of vasopressors to achieve a supraphysiological systolic blood pressure target. A single-centre retrospective, observational cohort study was undertaken at the Royal Adelaide Hospital intensive care unit. Data are presented as predominantly median (interquartile range (IQR)). All patients admitted with a diagnosis of aSAH between 1 April 2020 and 1 April 2022 were included and analysed according to whether they did or did not receive vasopressors for IH. A total of 109 patients were included, of which 29 (27%) received vasopressors for IH (median age 58 (IQR 52-65) years, 65% female) and 80 did not receive IH (median age 55 (IQR 49-71) years, 62% female). Clinical DCI or radiological evidence of vasospasm were present in all patients given IH and in 16% of non-IH patients. Patients in the IH group had more ischaemic electrocardiogram (ECG) changes (17.2% vs 2.5%, P = 0.01), urine output (4807 (IQR 3186-5720) ml/day vs 2125 (IQR 1650-2760) ml/day, P < 0.001), fluid administration (4895 (IQR 3555-5999) ml/day vs 2704 (IQR 2300-3403) ml/day, P < 0.001) and intravenous potassium replacement (13 (IQR 5-24) mmol/day vs 5 (IQR 0-13) mmol/day, P = 0.001) than those in the non-IH group. IH was also associated with a greater incidence of hyponatraemia (58% vs 34%, P = 0.02). IH was not associated with arrhythmias or rebleeding. Mortality rates were 17% vs 20% (P > 0.9) in the IH and non-IH groups respectively. In conclusion, IH for the treatment of DCI following aSAH was associated with an increased rate of ischaemic ECG changes, increased urine output and hyponatraemia. However, in the IH group there was no increased rate of rebleeding, and 48% of the IH patients had an improvement in their neurological function following commencement of treatment.
期刊介绍:
Anaesthesia and Intensive Care is an international journal publishing timely, peer reviewed articles that have educational value and scientific merit for clinicians and researchers associated with anaesthesia, intensive care medicine, and pain medicine.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


