Comparison of the oncological and functional outcomes among patients with high-risk upper tract urothelial cancer undergoing segmental ureterectomy based on tumour location
Abstract
Introduction
Segmental ureterectomy (SU) represents a viable alternative to radical nephroureterectomy (RNU) for the management of distal ureteral tumours when technically feasible. However, SU of the proximal two-thirds of the ureter is associated with higher failure rates compared to distal ureteral tumours. This study aims to compare oncologic outcomes and renal function in patients undergoing SU for tumours located in the distal versus proximal ureter.
Methods
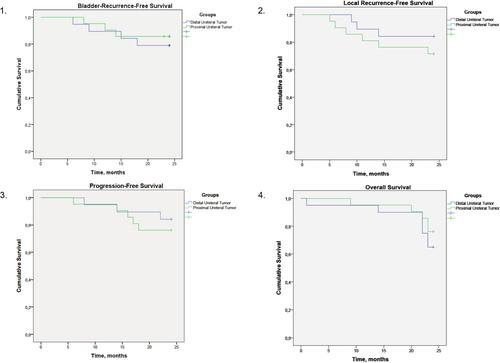
Prospective, non-randomized cohort study, which included adult patients with high-risk cT2–3 cN0–1 M0 ureteral tumours deemed suitable for SU, with preoperative affected kidney function > 15 ml/min. Patients were treated at a reference centre between March 2019 and March 2023. Patients were divided into two cohorts based on the primary tumour location: distal or proximal two-thirds of the ureter. All patients received neoadjuvant chemotherapy (Gem-Cis) and cases that underwent RNU were excluded from the study. Kaplan–Meier analysis was employed to evaluate local- recurrence-free survival (L-RFS), progression-free survival (PFS) and overall survival (OS).
Results
A total of 41 patients underwent SU (21/20 proximal/distal location). The cohorts were matched by age, sex, BMI, ECOG status, T-stage, pN status, tumour length, preoperative eGFR, primary pathology and positive cytology (p > 0.05). Following segmental ureterectomy, all patients with distal ureteral tumours underwent neostomy reconstruction. In the proximal ureter group, reconstruction techniques included end-to-end anastomosis in 9 (43%), Andersen-Heinz plasty in 8 (38%) and ureter-ileum interposition in 4 cases (19%).
No statistically significant differences were observed between the two cohorts in terms of surgery duration, average blood loss, Grade ≥3 complications, length of postoperative stay or 30-day readmission rate (p > 0.05). Postoperative eGFR was similar between the groups (60.4 ± 8.5 vs. 59.4 ± 11.4; p = 0.81). Furthermore, no significant differences were found between patients with proximal versus distal ureteral tumours in terms of 2-year L-RFS (72% vs. 85%; p = 0.29), PFS (85% vs. 77%; p = 0.69) or OS (65% vs. 77%; p = 0.43).
Conclusion
The current study demonstrates that segmental ureterectomy provides comparable oncologic outcomes and renal function preservation for both proximal and distal ureteral cancer. SU can be considered a safe and effective kidney-sparing alternative to radical nephroureterectomy in high-risk cases, regardless of tumour location.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


