Javier Alvarez-Galvez, Carolina Lagares-Franco, Esther Ortega-Martin, Helena De Sola, Antonio Rojas-García, Paloma Sanz-Marcos, José Almenara-Barrios, Angelos P Kassianos, Ilaria Montagni, María Camacho-García, Maribel Serrano-Macías, Jesús Carretero-Bravo
{"title":"Measurement, Characterization, and Mapping of COVID-19 Misinformation in Spain: Cross-Sectional Study.","authors":"Javier Alvarez-Galvez, Carolina Lagares-Franco, Esther Ortega-Martin, Helena De Sola, Antonio Rojas-García, Paloma Sanz-Marcos, José Almenara-Barrios, Angelos P Kassianos, Ilaria Montagni, María Camacho-García, Maribel Serrano-Macías, Jesús Carretero-Bravo","doi":"10.2196/69945","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The COVID-19 pandemic has been accompanied by an unprecedented infodemic characterized by the widespread dissemination of misinformation. Globally, misinformation about COVID-19 has led to polarized beliefs and behaviors, including vaccine hesitancy, rejection of governmental authorities' recommendations, and distrust in health institutions. Thus, understanding the prevalence and drivers of misinformation is critical for designing effective and contextualized public health strategies.</p><p><strong>Objective: </strong>On the basis of a tailored survey on health misinformation, this study aims to assess the prevalence and distribution of COVID-19-related misinformation in Spain; identify population groups based on their beliefs; and explore the social, economic, ideological, and media use factors associated with susceptibility to misinformation.</p><p><strong>Methods: </strong>A cross-sectional telephone survey was conducted with a nationally representative sample of 2200 individuals in Spain. The study developed the COVID-19 Misinformation Scale to measure beliefs in misinformation. Exploratory factor analysis identified key misinformation topics, and k-means clustering classified participants into 3 groups: convinced, hesitant, and skeptical. Multinomial logistic regression was used to explore associations between misinformation beliefs and demographic, social, and health-related variables.</p><p><strong>Results: </strong>Three population groups were identified: convinced (1078/2200, 49%), hesitant (666/2200, 30.27%), and skeptical (456/2200, 20.73%). Conspiracy theories, doubts about vaccines, and stories about sudden death emerged as the most endorsed current misinformation topics. Higher susceptibility to misinformation was associated with the female sex, lower socioeconomic status, use of low-quality information sources, higher levels of media sharing, greater religiosity, distrust of institutions, and extreme and unstated political ideologies. Frequent sharing of health information on social networks was also associated with membership in the skeptical group, regardless of whether the information was verified. Interestingly, women were prone to COVID-19 skepticism, a finding that warranted further research to understand the gender-specific factors driving vulnerability to health misinformation. In addition, a geographic distribution of hesitant and skeptical groups was observed that coincides with the so-called empty Spain, areas where political disaffection with the main political parties is greater.</p><p><strong>Conclusions: </strong>This study highlights the important role of determinants of susceptibility to COVID-19 misinformation that go beyond purely socioeconomic and ideological factors. Although these factors are relevant in explaining the social reproduction of this phenomenon, some determinants are linked to the use of social media (ie, searching and sharing of alternative health information) and probably the political disaffection of citizens who have stopped believing in both the ideologically centrist mainstream parties and the institutions that represent them. Furthermore, by establishing the profile and geographic distribution of the convinced, hesitant, and skeptical groups, our results provide useful insights for public health interventions. Specific strategies should focus on restoring institutional trust, promoting reliable sources of information, and addressing structural drivers of health misinformation linked to gender inequalities.</p>","PeriodicalId":73554,"journal":{"name":"JMIR infodemiology","volume":"5 ","pages":"e69945"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12209726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR infodemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/69945","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The COVID-19 pandemic has been accompanied by an unprecedented infodemic characterized by the widespread dissemination of misinformation. Globally, misinformation about COVID-19 has led to polarized beliefs and behaviors, including vaccine hesitancy, rejection of governmental authorities' recommendations, and distrust in health institutions. Thus, understanding the prevalence and drivers of misinformation is critical for designing effective and contextualized public health strategies.
Objective: On the basis of a tailored survey on health misinformation, this study aims to assess the prevalence and distribution of COVID-19-related misinformation in Spain; identify population groups based on their beliefs; and explore the social, economic, ideological, and media use factors associated with susceptibility to misinformation.
Methods: A cross-sectional telephone survey was conducted with a nationally representative sample of 2200 individuals in Spain. The study developed the COVID-19 Misinformation Scale to measure beliefs in misinformation. Exploratory factor analysis identified key misinformation topics, and k-means clustering classified participants into 3 groups: convinced, hesitant, and skeptical. Multinomial logistic regression was used to explore associations between misinformation beliefs and demographic, social, and health-related variables.
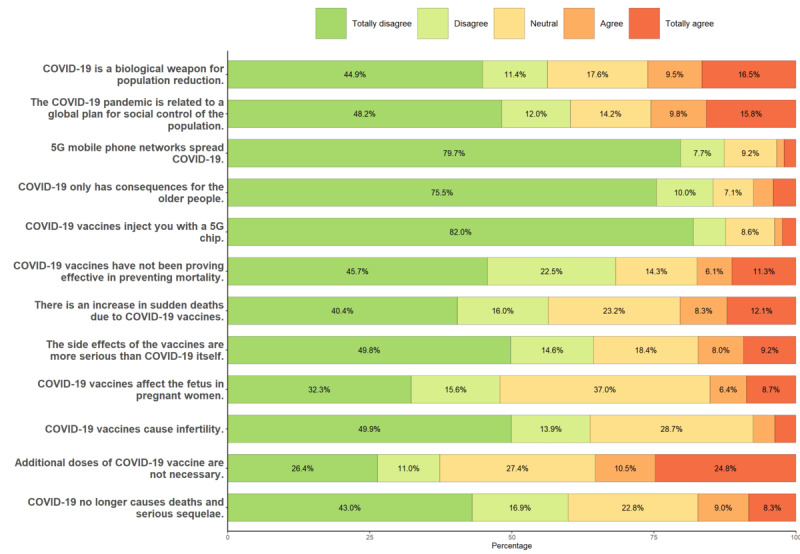
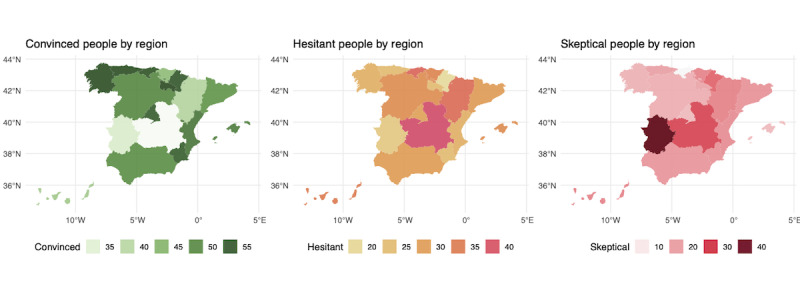
Results: Three population groups were identified: convinced (1078/2200, 49%), hesitant (666/2200, 30.27%), and skeptical (456/2200, 20.73%). Conspiracy theories, doubts about vaccines, and stories about sudden death emerged as the most endorsed current misinformation topics. Higher susceptibility to misinformation was associated with the female sex, lower socioeconomic status, use of low-quality information sources, higher levels of media sharing, greater religiosity, distrust of institutions, and extreme and unstated political ideologies. Frequent sharing of health information on social networks was also associated with membership in the skeptical group, regardless of whether the information was verified. Interestingly, women were prone to COVID-19 skepticism, a finding that warranted further research to understand the gender-specific factors driving vulnerability to health misinformation. In addition, a geographic distribution of hesitant and skeptical groups was observed that coincides with the so-called empty Spain, areas where political disaffection with the main political parties is greater.
Conclusions: This study highlights the important role of determinants of susceptibility to COVID-19 misinformation that go beyond purely socioeconomic and ideological factors. Although these factors are relevant in explaining the social reproduction of this phenomenon, some determinants are linked to the use of social media (ie, searching and sharing of alternative health information) and probably the political disaffection of citizens who have stopped believing in both the ideologically centrist mainstream parties and the institutions that represent them. Furthermore, by establishing the profile and geographic distribution of the convinced, hesitant, and skeptical groups, our results provide useful insights for public health interventions. Specific strategies should focus on restoring institutional trust, promoting reliable sources of information, and addressing structural drivers of health misinformation linked to gender inequalities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


