{"title":"Early Recurrence of Hepatocellular Carcinoma in Patients without Microscopic Vascular Invasion: Clinicopathological Characteristics and Risk Factors.","authors":"Hanh Thi Tuyet Ngo, Duy Duc Nguyen, Minh-Xuan Dang, Thao Thi Phuong Doan, Truc Thanh Thai","doi":"10.2147/JHC.S524683","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Early recurrence of hepatocellular carcinoma (HCC) is not uniformly associated with microscopic vascular invasion (MVI). This study aims to identify the clinical and pathological factors associated with early recurrence in HCC patients without MVI.</p><p><strong>Methods: </strong>A retrospective cohort study was conducted on 69 patients who underwent hepatectomy for HCC at the University Medical Center Ho Chi Minh city. All patients were microscopically confirmed as MVI-negative. Clinical and subclinical data, along with tumor recurrence within 24 months post-surgery were collected. Microscopic features of both tumor and non-tumor liver tissue were assessed using Hematoxylin-Eosin-stained slides.</p><p><strong>Results: </strong>The majority of patients were male (78.3%) and had cirrhosis (72.5%). The early recurrence rate was 31.9%, with most recurrences occurring between 6- and 18-month post-surgery. Independent factors for early tumor recurrence included preoperative treatment with Transarterial Chemoembolization (TACE) or Radiofrequency Ablation (RFA) (HR = 8.63, 95% CI = 1.45-51.38), tumor size > 5 cm (HR = 3.82, 95% CI = 1.17-12.42), and HCV infection (HR = 4.61, 95% CI = 1.41-15.1).</p><p><strong>Conclusion: </strong>The pathogenesis and pattern of early tumor recurrence in MVI-negative HCC differ from that in MVI-positive cases. Identifying risk factors, such as HCV infection, tumor size, and preoperative locoregional therapy, may aid in optimizing treatment strategies and postoperative surveillance.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1167-1175"},"PeriodicalIF":3.4000,"publicationDate":"2025-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12168972/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S524683","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Early recurrence of hepatocellular carcinoma (HCC) is not uniformly associated with microscopic vascular invasion (MVI). This study aims to identify the clinical and pathological factors associated with early recurrence in HCC patients without MVI.
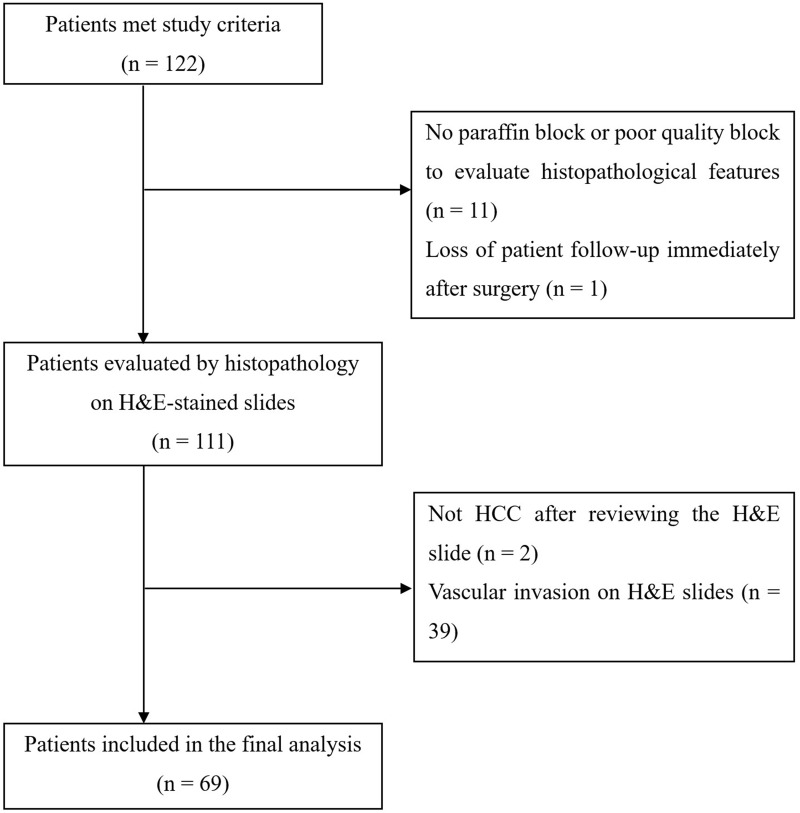
Methods: A retrospective cohort study was conducted on 69 patients who underwent hepatectomy for HCC at the University Medical Center Ho Chi Minh city. All patients were microscopically confirmed as MVI-negative. Clinical and subclinical data, along with tumor recurrence within 24 months post-surgery were collected. Microscopic features of both tumor and non-tumor liver tissue were assessed using Hematoxylin-Eosin-stained slides.
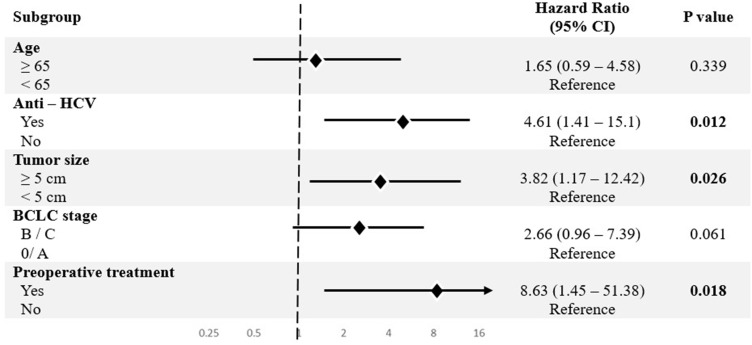
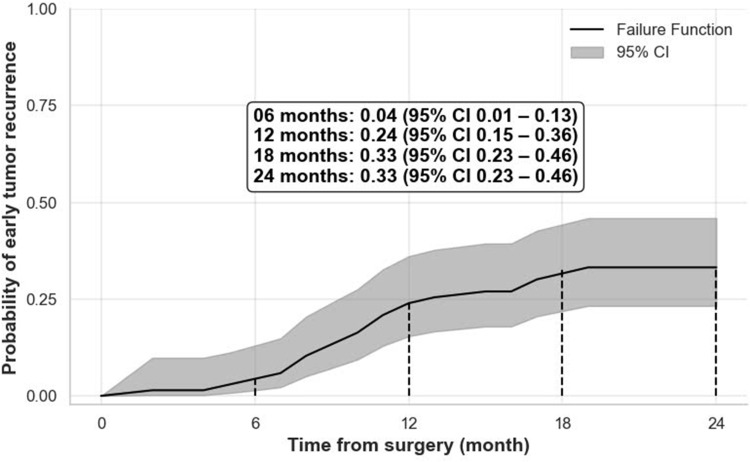
Results: The majority of patients were male (78.3%) and had cirrhosis (72.5%). The early recurrence rate was 31.9%, with most recurrences occurring between 6- and 18-month post-surgery. Independent factors for early tumor recurrence included preoperative treatment with Transarterial Chemoembolization (TACE) or Radiofrequency Ablation (RFA) (HR = 8.63, 95% CI = 1.45-51.38), tumor size > 5 cm (HR = 3.82, 95% CI = 1.17-12.42), and HCV infection (HR = 4.61, 95% CI = 1.41-15.1).
Conclusion: The pathogenesis and pattern of early tumor recurrence in MVI-negative HCC differ from that in MVI-positive cases. Identifying risk factors, such as HCV infection, tumor size, and preoperative locoregional therapy, may aid in optimizing treatment strategies and postoperative surveillance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


