{"title":"A Case Report of Dialysis Catheter Placement in an Anomalous Pulmonary Vein.","authors":"Cierra King, Karling Gravenstein","doi":"10.1155/crvm/9936069","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Partial anomalous pulmonary venous connections are embryologic defects in which the normal connection between the pulmonary veins and left atrium is disrupted. These rare anomalies are often asymptomatic and identified incidentally. The most common variant is a connection between the left upper pulmonary veins and the left innominate vein. Although typically asymptomatic, these variants are important to be aware of, particularly when performing procedures involving the venous anatomy. <b>Case Presentation:</b> We present the case of a 52-year-old female with a previous history of colon cancer who underwent right hemicolectomy and presented to the hospital due to severe dehydration secondary to profuse nausea, vomiting, and diarrhea. She developed an acute kidney injury with electrolyte derangement and metabolic acidosis requiring initiation of hemodialysis. Due to her preexisting right internal jugular port access, the decision was made to proceed with left internal jugular dialysis catheter access. Central venous access was performed in standard fashion. There was venous-appearing blood return at the time of needle access and subsequent dilations. However, at the time of catheter advancement, there was noted return of bright red blood and resistance to advancement, concerning for possible arterial cannulation. Concerning arterial placement, an arterial blood gas (ABG) test and chest x-ray were performed; however, the transducer waveforms were not consistent with this. Computed tomography angiography obtained revealed left internal jugular venous access with catheter extension into an anomalous pulmonary vein within the left upper lobe. The patient was taken to the angiography suite and under fluoroscopy guidance had new left internal jugular catheter access with the catheter terminating successfully in the superior vena cava. She underwent successful dialysis and was subsequently discharged on postprocedure Day 8. <b>Conclusions:</b> Central line placement is a commonly performed procedure in hospitals. There are steps that have been developed to limit complications for this procedure, including ultrasound guidance, visualization of venous blood, and confirmatory imaging prior to use. This is a case in which arterial-appearing blood, paO2, and chest x-ray were concerning for incorrect placement, but additional imaging revealed accurate access with anomalous anatomy. Overall, the case of central line placement in anomalous pulmonary venous connections is rare but needs consideration when the clinical scenario is appropriate.</p>","PeriodicalId":9632,"journal":{"name":"Case Reports in Vascular Medicine","volume":"2025 ","pages":"9936069"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12170080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Vascular Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crvm/9936069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
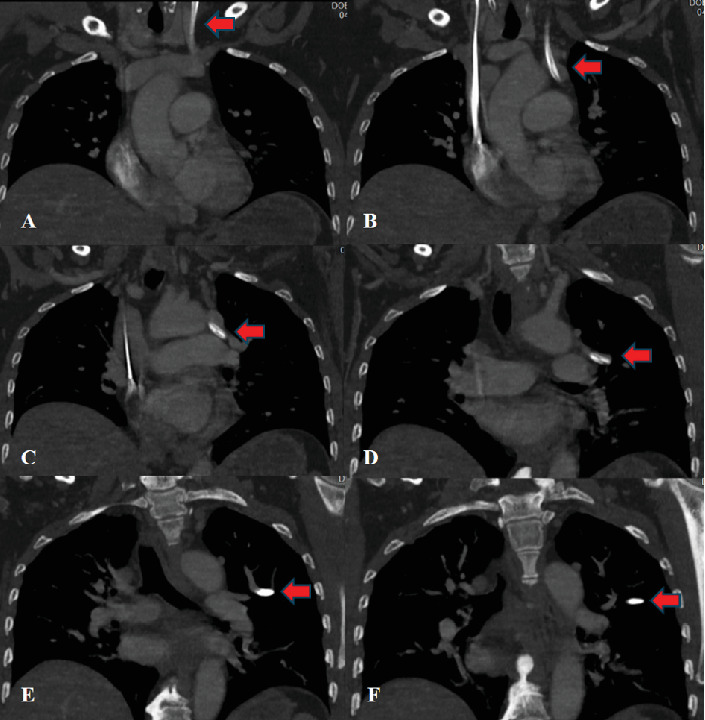
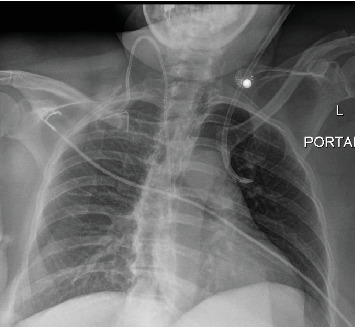
Background: Partial anomalous pulmonary venous connections are embryologic defects in which the normal connection between the pulmonary veins and left atrium is disrupted. These rare anomalies are often asymptomatic and identified incidentally. The most common variant is a connection between the left upper pulmonary veins and the left innominate vein. Although typically asymptomatic, these variants are important to be aware of, particularly when performing procedures involving the venous anatomy. Case Presentation: We present the case of a 52-year-old female with a previous history of colon cancer who underwent right hemicolectomy and presented to the hospital due to severe dehydration secondary to profuse nausea, vomiting, and diarrhea. She developed an acute kidney injury with electrolyte derangement and metabolic acidosis requiring initiation of hemodialysis. Due to her preexisting right internal jugular port access, the decision was made to proceed with left internal jugular dialysis catheter access. Central venous access was performed in standard fashion. There was venous-appearing blood return at the time of needle access and subsequent dilations. However, at the time of catheter advancement, there was noted return of bright red blood and resistance to advancement, concerning for possible arterial cannulation. Concerning arterial placement, an arterial blood gas (ABG) test and chest x-ray were performed; however, the transducer waveforms were not consistent with this. Computed tomography angiography obtained revealed left internal jugular venous access with catheter extension into an anomalous pulmonary vein within the left upper lobe. The patient was taken to the angiography suite and under fluoroscopy guidance had new left internal jugular catheter access with the catheter terminating successfully in the superior vena cava. She underwent successful dialysis and was subsequently discharged on postprocedure Day 8. Conclusions: Central line placement is a commonly performed procedure in hospitals. There are steps that have been developed to limit complications for this procedure, including ultrasound guidance, visualization of venous blood, and confirmatory imaging prior to use. This is a case in which arterial-appearing blood, paO2, and chest x-ray were concerning for incorrect placement, but additional imaging revealed accurate access with anomalous anatomy. Overall, the case of central line placement in anomalous pulmonary venous connections is rare but needs consideration when the clinical scenario is appropriate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


