Proximal humeral endoprosthetic reconstruction for tumour defects : clinical outcomes of 165 patients from the MUTARS Orthopedic Registry Orthopedic Registry Europe (MORE).
Richard Evenhuis, Michaël P A Bus, Simen Sellevold, Edwin F Dierselhuis, Ioannis G Trikoupis, Maurizio Scorianz, Sebastian Walter, Jorge Cabrolier, Marta Fiocco, Michiel A J van de Sande
{"title":"Proximal humeral endoprosthetic reconstruction for tumour defects : clinical outcomes of 165 patients from the MUTARS Orthopedic Registry Orthopedic Registry Europe (MORE).","authors":"Richard Evenhuis, Michaël P A Bus, Simen Sellevold, Edwin F Dierselhuis, Ioannis G Trikoupis, Maurizio Scorianz, Sebastian Walter, Jorge Cabrolier, Marta Fiocco, Michiel A J van de Sande","doi":"10.1302/2633-1462.66.BJO-2025-0018","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Tumour defects of the proximal humerus can be reconstructed using hemiarthroplasty, reverse shoulder arthroplasty (RSA), or anatomical total shoulder arthroplasty (TSA). This study aimed to evaluate clinical and functional outcomes of reconstructions of proximal humeral tumour defects with MUTARS endoprostheses.</p><p><strong>Methods: </strong>A total of 165 reconstructions were included: 98 (59%) hemiarthroplasties, 61 (37%) RSAs, and six (4%) TSAs. Median age was 54 years (IQR 31 to 68). Median follow-up time was 5.9 years (IQR 2.83 to 10.50). Competing risks models were employed to estimate the cumulative incidence of revision (CIR) for mechanical reasons and infection with local recurrence and mortality as competing events. The range of motion was reported using descriptive statistics.</p><p><strong>Results: </strong>Axillary nerve preservation and deltoid muscle reattachment were observed in 89% and 96% of cases, respectively, without significant differences between implant types. Rotator cuff refixation was less frequent in RSA (78%) compared to hemiarthroplasty (91%). Overall, 26 implants (16%) were revised for mechanical complications (dislocation n = 11, loosening n = 2, periprosthetic fracture n = 3) and infection (n = 10). Patients with previous surgery at the same site had a higher revision risk due to instability (cause-specific hazard ratio 3.7; 95% CI 1.3 to 10.8). The CIRs for mechanical reasons (Henderson 1 to 3) in the entire population at two, five, and ten years were 7% (95% CI 3 to 11), 11% (95% CI 6 to 17), and 13% (95% CI 7 to 20), respectively. For periprosthetic joint infection (Henderson 4), the CIRs were 5% (95% CI 2 to 10), 7% (95% CI 3 to 12), and 7% (95% CI 3 to 12). Compared with hemiarthroplasty, RSA offered superior median anteflexion (73° (IQR 40 to 90) vs 30° (IQR 5 to 45)), abduction (70° (IQR 38 to 90) vs 30° (IQR 5 to 45)), and external rotation (15° (IQR 0 to 28) vs 5° (0 to 19)).</p><p><strong>Conclusion: </strong>MUTARS proximal humerus reconstruction outcomes are satisfying, particularly in terms of mechanical failure. RSA and hemiarthroplasty exhibit comparable revision risks, with previous surgery at same site as a prognostic factor for revision due to dislocation. RSA appears to provide the best functional outcome.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 6","pages":"715-723"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167655/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.66.BJO-2025-0018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Tumour defects of the proximal humerus can be reconstructed using hemiarthroplasty, reverse shoulder arthroplasty (RSA), or anatomical total shoulder arthroplasty (TSA). This study aimed to evaluate clinical and functional outcomes of reconstructions of proximal humeral tumour defects with MUTARS endoprostheses.
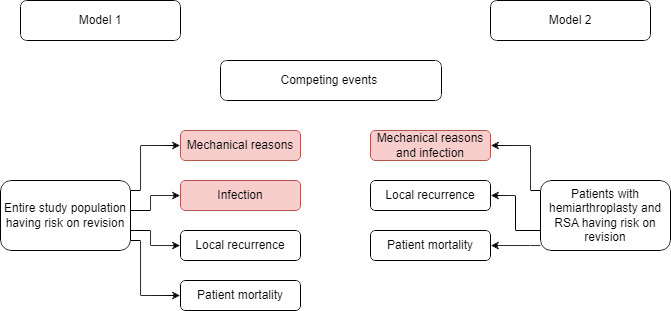
Methods: A total of 165 reconstructions were included: 98 (59%) hemiarthroplasties, 61 (37%) RSAs, and six (4%) TSAs. Median age was 54 years (IQR 31 to 68). Median follow-up time was 5.9 years (IQR 2.83 to 10.50). Competing risks models were employed to estimate the cumulative incidence of revision (CIR) for mechanical reasons and infection with local recurrence and mortality as competing events. The range of motion was reported using descriptive statistics.
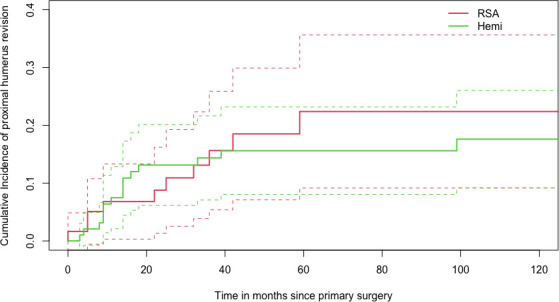
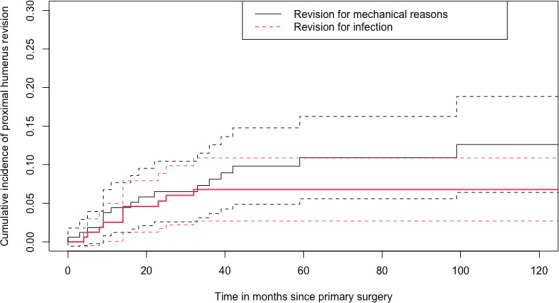
Results: Axillary nerve preservation and deltoid muscle reattachment were observed in 89% and 96% of cases, respectively, without significant differences between implant types. Rotator cuff refixation was less frequent in RSA (78%) compared to hemiarthroplasty (91%). Overall, 26 implants (16%) were revised for mechanical complications (dislocation n = 11, loosening n = 2, periprosthetic fracture n = 3) and infection (n = 10). Patients with previous surgery at the same site had a higher revision risk due to instability (cause-specific hazard ratio 3.7; 95% CI 1.3 to 10.8). The CIRs for mechanical reasons (Henderson 1 to 3) in the entire population at two, five, and ten years were 7% (95% CI 3 to 11), 11% (95% CI 6 to 17), and 13% (95% CI 7 to 20), respectively. For periprosthetic joint infection (Henderson 4), the CIRs were 5% (95% CI 2 to 10), 7% (95% CI 3 to 12), and 7% (95% CI 3 to 12). Compared with hemiarthroplasty, RSA offered superior median anteflexion (73° (IQR 40 to 90) vs 30° (IQR 5 to 45)), abduction (70° (IQR 38 to 90) vs 30° (IQR 5 to 45)), and external rotation (15° (IQR 0 to 28) vs 5° (0 to 19)).
Conclusion: MUTARS proximal humerus reconstruction outcomes are satisfying, particularly in terms of mechanical failure. RSA and hemiarthroplasty exhibit comparable revision risks, with previous surgery at same site as a prognostic factor for revision due to dislocation. RSA appears to provide the best functional outcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


