{"title":"Large Hematoma Following Ultrasound-Guided Rectus Sheath Block.","authors":"Toshie Shiraishi","doi":"10.2147/LRA.S511201","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Rectus sheath block is a commonly used nerve block to reduce pain from abdominal surgery. Although hematoma complications due to vascular injury during nerve block is rare, it remains an important consideration, particularly in cases requiring the use of antithrombogenic agents. In rectus sheath block, anesthesiologists are aware that major vessels subject to needle puncture injury during the procedure include the inferior epigastric artery (IEA) and inferior epigastric vein (IEV). However, increasing use of ultrasound-guided block has resulted in a decrease in significant bleeding risk, including in patients taking antithrombogenic agents. We recently experienced a large subcutaneous hematoma (430 mL) after rectus sheath block. In this case report, we describe the clinical course of the hematoma and discuss its cause and the possible vessels involved, including the IEA and IEV, and branches such as the superior epigastric arteries and veins.</p><p><strong>Case presentation: </strong>A 40-year-old female underwent bilateral ultrasound-guided rectus sheath block and transversus abdominis block following laparoscopic cholecystectomy. After the operation, a large, painful hematoma was identified with a volume estimated at 430 mL. Investigation of the bleeding site by CT scan showed that the hematoma was subcutaneous and in an area with multiple venous and arterial branches. Identification of the responsible vessel appeared difficult; however, on discussion with the radiologist, bleeding from a cutaneous (or deeper) vessel from the block or surgical (trocar or needle) injury was included in the different diagnosis. The superficial epigastric artery was considered the most probable source because it was the closest to the hematoma.</p><p><strong>Conclusion: </strong>Although the IEA and IEV are the major candidates for vascular injury in rectus sheath block, clinicians should recognize that the SEA can also be injured during rectus sheath block procedures.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"18 ","pages":"39-44"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12164880/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S511201","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
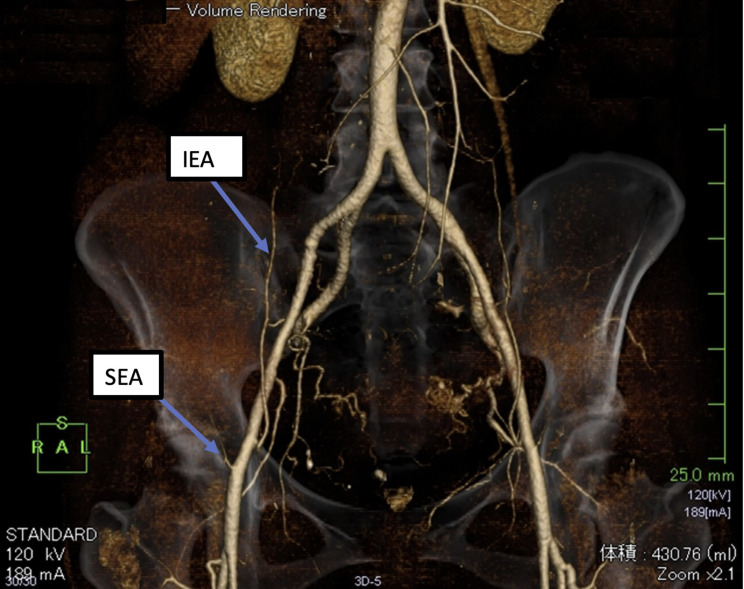
Purpose: Rectus sheath block is a commonly used nerve block to reduce pain from abdominal surgery. Although hematoma complications due to vascular injury during nerve block is rare, it remains an important consideration, particularly in cases requiring the use of antithrombogenic agents. In rectus sheath block, anesthesiologists are aware that major vessels subject to needle puncture injury during the procedure include the inferior epigastric artery (IEA) and inferior epigastric vein (IEV). However, increasing use of ultrasound-guided block has resulted in a decrease in significant bleeding risk, including in patients taking antithrombogenic agents. We recently experienced a large subcutaneous hematoma (430 mL) after rectus sheath block. In this case report, we describe the clinical course of the hematoma and discuss its cause and the possible vessels involved, including the IEA and IEV, and branches such as the superior epigastric arteries and veins.
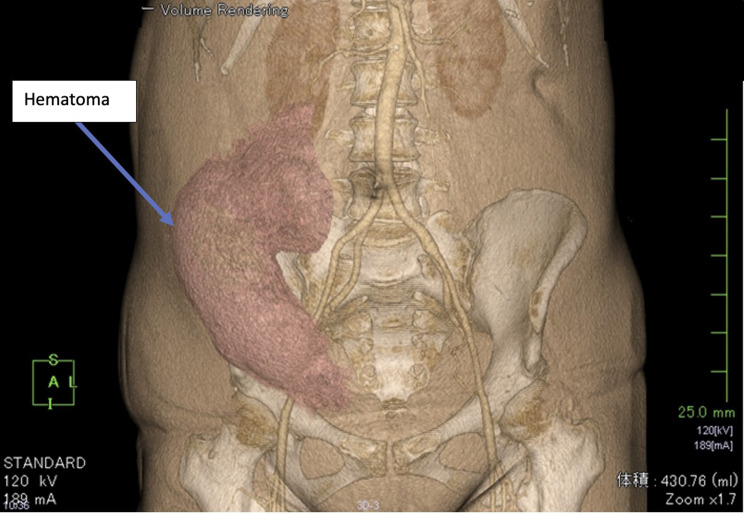
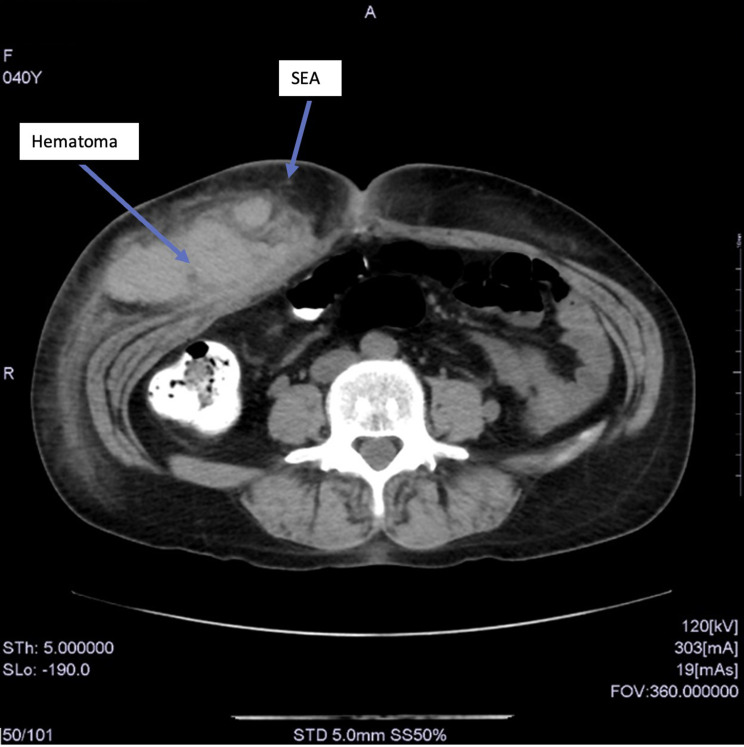
Case presentation: A 40-year-old female underwent bilateral ultrasound-guided rectus sheath block and transversus abdominis block following laparoscopic cholecystectomy. After the operation, a large, painful hematoma was identified with a volume estimated at 430 mL. Investigation of the bleeding site by CT scan showed that the hematoma was subcutaneous and in an area with multiple venous and arterial branches. Identification of the responsible vessel appeared difficult; however, on discussion with the radiologist, bleeding from a cutaneous (or deeper) vessel from the block or surgical (trocar or needle) injury was included in the different diagnosis. The superficial epigastric artery was considered the most probable source because it was the closest to the hematoma.
Conclusion: Although the IEA and IEV are the major candidates for vascular injury in rectus sheath block, clinicians should recognize that the SEA can also be injured during rectus sheath block procedures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


