Maria Wobith, C Oberhoffner, A Müller, M Fischer, M Lurz, B Jansen-Winkeln, A Weimann
{"title":"Individual multimodal prehabilitation in high-risk patients undergoing major abdominal surgery following neoadjuvant treatment - a feasibility study.","authors":"Maria Wobith, C Oberhoffner, A Müller, M Fischer, M Lurz, B Jansen-Winkeln, A Weimann","doi":"10.1007/s00423-025-03717-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Despite advancements in medicine, perioperative complications and functional decline remain challenges for patients undergoing major abdominal surgery, particularly in high-risk individuals with limited functional capacity and impaired nutritional status. Prehabilitation, which involves interventions before surgery, shows promise in addressing these issues, but the heterogeneity of studies limits specific recommendations. The integration of prehabilitation into clinical practice with special regard to the setting and modalities of treatment also remain unclear.</p><p><strong>Methods: </strong>As a feasibility study for home-based prehabilitation high-risk patients (age ≥ 70 years, ASA ≥ 3) undergoing neoadjuvant treatment for non-metastatic esophageal, gastric, or rectal cancer, followed by oncological resection were included. A six-week multimodal supervised home-based prehabilitation program, including nutritional therapy, exercise, and psychological support, was implemented after neoadjuvant treatment and before surgery. Functional, nutritional, and quality of life (QoL) assessments were conducted at multiple points. Feasibility and adherence were assessed. Secondary explorative outcome measures included complication rates, hospital stay, readmission, and mortality, which were compared to a matched cohort.</p><p><strong>Results: </strong>Of 24 enrolled patients, 20 completed the program, with high adherence to home-based workouts (91.8%), respiratory exercises (92.9%), and oral nutritional supplements (ONS) (88.7%). Functional and nutritional improvements were observed, including improved sit-to-stand performance (p = 0.025) and serum albumin levels (p = 0.001). QoL improved in the physical function domain (p = 0.009). Postoperative outcomes were similar between groups.</p><p><strong>Conclusion: </strong>A supervised home-based prehabilitation program is feasible for high-risk patients, with high adherence to interventions and potential benefits in functional and nutritional status. Further research is needed to optimize program content, identify optimal patient populations, and assess long-term outcomes.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"197"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12170726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03717-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Despite advancements in medicine, perioperative complications and functional decline remain challenges for patients undergoing major abdominal surgery, particularly in high-risk individuals with limited functional capacity and impaired nutritional status. Prehabilitation, which involves interventions before surgery, shows promise in addressing these issues, but the heterogeneity of studies limits specific recommendations. The integration of prehabilitation into clinical practice with special regard to the setting and modalities of treatment also remain unclear.
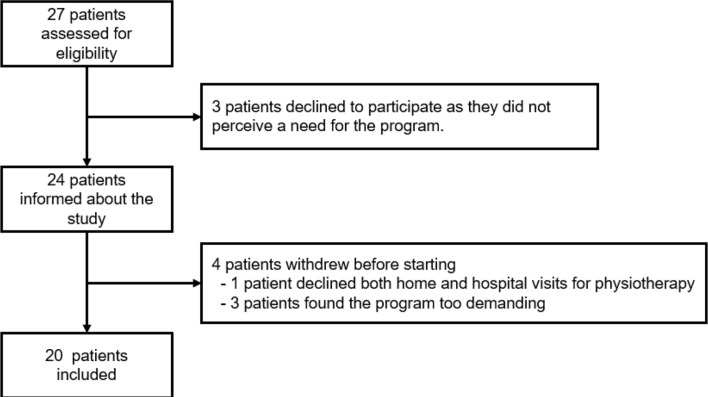
Methods: As a feasibility study for home-based prehabilitation high-risk patients (age ≥ 70 years, ASA ≥ 3) undergoing neoadjuvant treatment for non-metastatic esophageal, gastric, or rectal cancer, followed by oncological resection were included. A six-week multimodal supervised home-based prehabilitation program, including nutritional therapy, exercise, and psychological support, was implemented after neoadjuvant treatment and before surgery. Functional, nutritional, and quality of life (QoL) assessments were conducted at multiple points. Feasibility and adherence were assessed. Secondary explorative outcome measures included complication rates, hospital stay, readmission, and mortality, which were compared to a matched cohort.
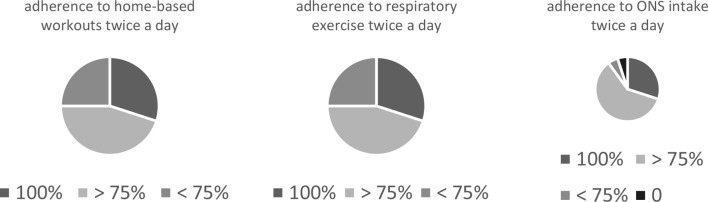
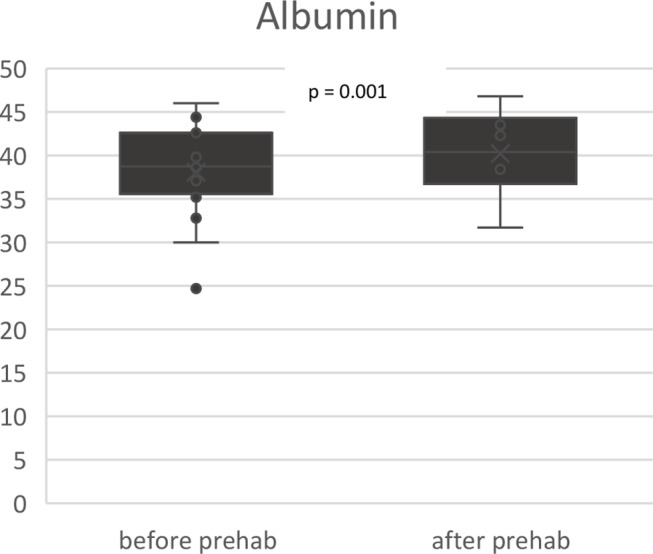
Results: Of 24 enrolled patients, 20 completed the program, with high adherence to home-based workouts (91.8%), respiratory exercises (92.9%), and oral nutritional supplements (ONS) (88.7%). Functional and nutritional improvements were observed, including improved sit-to-stand performance (p = 0.025) and serum albumin levels (p = 0.001). QoL improved in the physical function domain (p = 0.009). Postoperative outcomes were similar between groups.
Conclusion: A supervised home-based prehabilitation program is feasible for high-risk patients, with high adherence to interventions and potential benefits in functional and nutritional status. Further research is needed to optimize program content, identify optimal patient populations, and assess long-term outcomes.
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


