Cosmin Balan, Bianca Morosanu, Antonia Fodoroiu, Vlad Dobre, Andrei Dumitrache, Robert Thomas Barbulescu, Liana Valeanu, Cornel Robu, Cristian Boros, Alexandru Nica, Adrian Wong, Francesco Corradi, Ioana Marina Grintescu, Serban-Ion Bubenek-Turconi
{"title":"Decoding portal vein pulsatility: hemodynamic determinants in a post-hoc analysis of a prospective observational trial.","authors":"Cosmin Balan, Bianca Morosanu, Antonia Fodoroiu, Vlad Dobre, Andrei Dumitrache, Robert Thomas Barbulescu, Liana Valeanu, Cornel Robu, Cristian Boros, Alexandru Nica, Adrian Wong, Francesco Corradi, Ioana Marina Grintescu, Serban-Ion Bubenek-Turconi","doi":"10.1186/s13613-025-01498-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The portal vein pulsatility index (PVPI) reflects systemic congestion and is influenced by both volume status and right ventricular (RV) function. The mean systemic filling pressure analogue (Pmsa), derived from a mathematical model, estimates the interaction between stressed blood volume and systemic vascular compliance, serving as surrogate marker of volume status. This post-hoc analysis of an observational trial investigates the combined role of Pmsa and RV function as determinants of PVPI using echocardiography. Fifty-five mechanically ventilated patients with circulatory failure were included within 6 h of ICU admission following elective open-heart surgery. Fluid-tolerant patients (PVPI < 50%) underwent a passive leg raising (PLR) test; fluid-responsive patients subsequently received 7 mL/kg of Ringer's lactate. PVPI and Pmsa were measured at five timepoints: baseline (T1), after PLR (T2), upon returning to baseline (T3), after fluid administration (T4), and 20 min post-infusion (T5). RV function parameters, including RV to LV end-diastolic area ratio (RVEDA/LVEDA), tricuspid lateral annular systolic velocity (RV S'), RV fractional area change (RVFAC), pulmonary acceleration time (PAT), and right myocardial performance index (RIMP)-were assessed at T1, T4, and T5. Only fluid-responsive patients were evaluated beyond T3.</p><p><strong>Results: </strong>At T1, robust multilinear regression including all patients identified RVEDA/LVEDA (β = 10.38; p < 0.001), RIMP (β = - 6.54; p = 0.002), and RV S' (β = - 0.60; p = 0.002) as significant determinants of squared PVPI. In all patients, repeated measures correlation between Pmsa and PVPI was strong across T1-to-T3 (ρ = 0.785; p < 0.001), increasing from a non-significant correlation at T1 (ρ = 0.215; p = 0.115). Generalized estimating equations conducted only in fluid-responsive patients across T1, T4, and T5 identified Pmsa (β = 4.19; p < 0.001), RV S' (β = - 5.84; p < 0.001), RVEDA/LVEDA (β = 34.85; p = 0.018), and RIMP (β = - 35.28; p = 0.039) as significant determinants of PVPI.</p><p><strong>Conclusion: </strong>RV function and Pmsa are key determinants of PVPI. Their combined assessment may support an individualized congestion management by guiding interventions toward volume status, RV function, or both. Trial registration Primary Trial Registration: NCT06440772. Registered 30 May 2024. Retrospectively registered.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"81"},"PeriodicalIF":5.5000,"publicationDate":"2025-06-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167214/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01498-0","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The portal vein pulsatility index (PVPI) reflects systemic congestion and is influenced by both volume status and right ventricular (RV) function. The mean systemic filling pressure analogue (Pmsa), derived from a mathematical model, estimates the interaction between stressed blood volume and systemic vascular compliance, serving as surrogate marker of volume status. This post-hoc analysis of an observational trial investigates the combined role of Pmsa and RV function as determinants of PVPI using echocardiography. Fifty-five mechanically ventilated patients with circulatory failure were included within 6 h of ICU admission following elective open-heart surgery. Fluid-tolerant patients (PVPI < 50%) underwent a passive leg raising (PLR) test; fluid-responsive patients subsequently received 7 mL/kg of Ringer's lactate. PVPI and Pmsa were measured at five timepoints: baseline (T1), after PLR (T2), upon returning to baseline (T3), after fluid administration (T4), and 20 min post-infusion (T5). RV function parameters, including RV to LV end-diastolic area ratio (RVEDA/LVEDA), tricuspid lateral annular systolic velocity (RV S'), RV fractional area change (RVFAC), pulmonary acceleration time (PAT), and right myocardial performance index (RIMP)-were assessed at T1, T4, and T5. Only fluid-responsive patients were evaluated beyond T3.
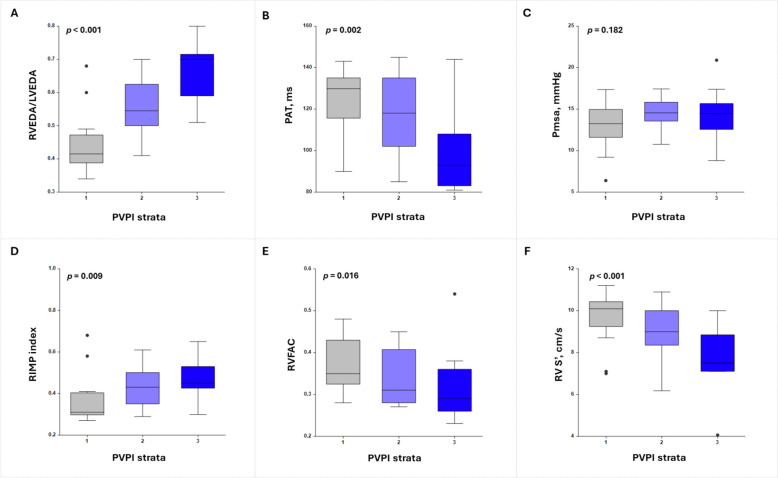
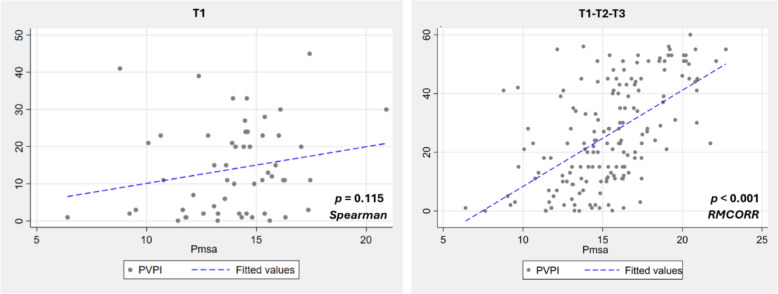
Results: At T1, robust multilinear regression including all patients identified RVEDA/LVEDA (β = 10.38; p < 0.001), RIMP (β = - 6.54; p = 0.002), and RV S' (β = - 0.60; p = 0.002) as significant determinants of squared PVPI. In all patients, repeated measures correlation between Pmsa and PVPI was strong across T1-to-T3 (ρ = 0.785; p < 0.001), increasing from a non-significant correlation at T1 (ρ = 0.215; p = 0.115). Generalized estimating equations conducted only in fluid-responsive patients across T1, T4, and T5 identified Pmsa (β = 4.19; p < 0.001), RV S' (β = - 5.84; p < 0.001), RVEDA/LVEDA (β = 34.85; p = 0.018), and RIMP (β = - 35.28; p = 0.039) as significant determinants of PVPI.
Conclusion: RV function and Pmsa are key determinants of PVPI. Their combined assessment may support an individualized congestion management by guiding interventions toward volume status, RV function, or both. Trial registration Primary Trial Registration: NCT06440772. Registered 30 May 2024. Retrospectively registered.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


