Rachel B Ger, Anh Tran, Victoria J Croog, Lawrence R Kleinberg, Carmen Kut, Brandi R Page, Kristin J Redmond, Heng Li
{"title":"Optimizing QACT Frequency and Setup Uncertainty in Cranial Proton Therapy for Normal Tissue Sparing.","authors":"Rachel B Ger, Anh Tran, Victoria J Croog, Lawrence R Kleinberg, Carmen Kut, Brandi R Page, Kristin J Redmond, Heng Li","doi":"10.1016/j.ijpt.2025.100751","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Proton therapy offers superior conformality in cranial dose distributions, but its sensitivity to anatomical air-tissue interfaces and patient setup variations can compromise dosimetric robustness. Quality assurance computed tomography (QACT) scans can verify these changes, though they increase cumulative dose and workflow burden. There are currently gaps in knowledge about the setup uncertainty margin that could maintain acceptable daily target coverage, organ at risk (OAR) sparing, and QACT frequency requirements.</p><p><strong>Materials and methods: </strong>A total of 122 adult patients treated for cranial targets between 2019 and 2023 were retrospectively reviewed. Patients were analyzed for adaptive planning rates based on if they had beams passing through the neck or not, and if beams passed through the nasal cavity or not. Twenty patients that did not have beams passing through the neck or nasal cavity were randomly selected and replanned using 2 mm setup uncertainty for robustness compared to the clinically utilized 3 mm setup uncertainty. Synthetic CTs were created for each daily cone beam CT, and the clinical goals were compared against the robustness expectations.</p><p><strong>Results: </strong>Six patients had adaptive plans, only 2 of which were due to anatomical changes, and both of these patients had beams passing through the nasal cavity. Volumetric clinical goals for the clinical target volume (CTV) were met in 95.7% and 99.6% of 2 and 3 mm plans, respectively. Maximum deviation for 2 mm plans was -0.3%. Clinical goals were met in 99.3% of both 2 and 3 mm plans. All dose differences were below 50 cGy except for 1 patient.</p><p><strong>Conclusion: </strong>The implementation of a tailored QACT schedule based on beam trajectory and target location is supported, reducing unnecessary imaging without compromising treatment accuracy recommending a single QACT for all patients except those with targets traversing the sinuses or bulky surface targets. A 2 mm setup uncertainty was shown to provide robust target coverage while minimizing OAR dose.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"16 ","pages":"100751"},"PeriodicalIF":2.0000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12162028/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.ijpt.2025.100751","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Proton therapy offers superior conformality in cranial dose distributions, but its sensitivity to anatomical air-tissue interfaces and patient setup variations can compromise dosimetric robustness. Quality assurance computed tomography (QACT) scans can verify these changes, though they increase cumulative dose and workflow burden. There are currently gaps in knowledge about the setup uncertainty margin that could maintain acceptable daily target coverage, organ at risk (OAR) sparing, and QACT frequency requirements.
Materials and methods: A total of 122 adult patients treated for cranial targets between 2019 and 2023 were retrospectively reviewed. Patients were analyzed for adaptive planning rates based on if they had beams passing through the neck or not, and if beams passed through the nasal cavity or not. Twenty patients that did not have beams passing through the neck or nasal cavity were randomly selected and replanned using 2 mm setup uncertainty for robustness compared to the clinically utilized 3 mm setup uncertainty. Synthetic CTs were created for each daily cone beam CT, and the clinical goals were compared against the robustness expectations.
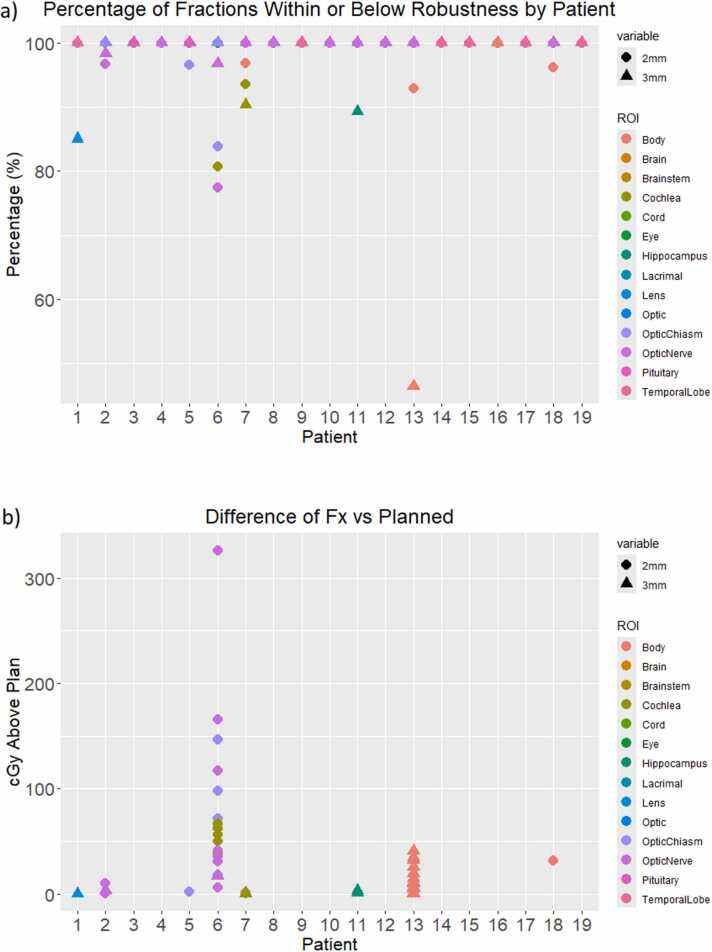
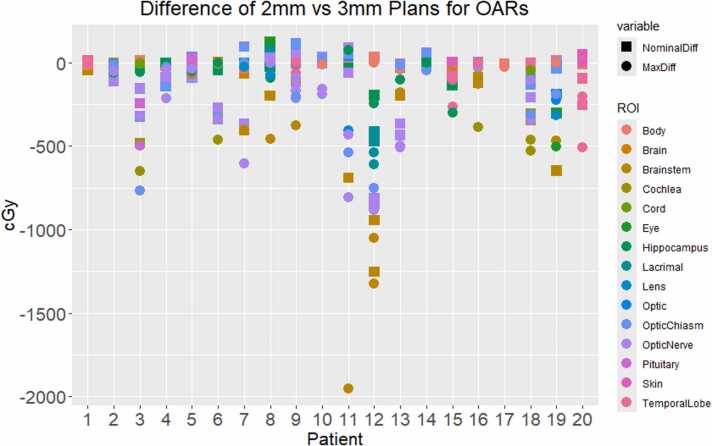
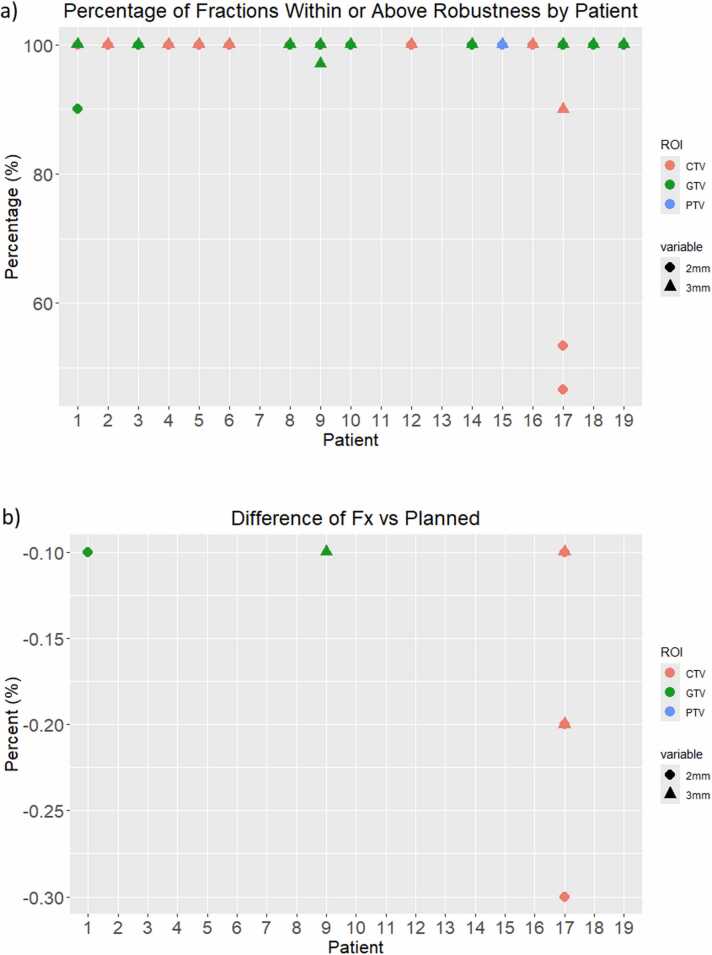
Results: Six patients had adaptive plans, only 2 of which were due to anatomical changes, and both of these patients had beams passing through the nasal cavity. Volumetric clinical goals for the clinical target volume (CTV) were met in 95.7% and 99.6% of 2 and 3 mm plans, respectively. Maximum deviation for 2 mm plans was -0.3%. Clinical goals were met in 99.3% of both 2 and 3 mm plans. All dose differences were below 50 cGy except for 1 patient.
Conclusion: The implementation of a tailored QACT schedule based on beam trajectory and target location is supported, reducing unnecessary imaging without compromising treatment accuracy recommending a single QACT for all patients except those with targets traversing the sinuses or bulky surface targets. A 2 mm setup uncertainty was shown to provide robust target coverage while minimizing OAR dose.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


