Discriminating Disease Flare From Infection in Febrile Patients With Systemic Lupus Erythematosus in a Safety-Net Hospital System: A Multicenter Study.
Abhimanyu Amarnani, Flora Liu, Melissa Lee Wilson, Nathan Lim, William Stohl, Leanna Wise
{"title":"Discriminating Disease Flare From Infection in Febrile Patients With Systemic Lupus Erythematosus in a Safety-Net Hospital System: A Multicenter Study.","authors":"Abhimanyu Amarnani, Flora Liu, Melissa Lee Wilson, Nathan Lim, William Stohl, Leanna Wise","doi":"10.1002/acr2.70051","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The objective of this study was to assess clinical laboratory parameters that distinguish between disease flare and infection in febrile patients with systemic lupus erythematosus (SLE) at safety-net hospitals in Los Angeles.</p><p><strong>Methods: </strong>We reviewed electronic medical records of patients admitted from August 1, 2016, through July 31, 2019, categorizing them as disease flare, bacterial infection (culture positive), culture-negative infection, and both flare and infection. Laboratory parameters collected within 48 hours of admission (complete blood cell count with differential, liver function panel, erythrocyte sedimentation rate [ESR], C-reactive protein [CRP], C3, C4, lactate, procalcitonin, and ferritin) were analyzed.</p><p><strong>Results: </strong>Several laboratory parameters significantly distinguished febrile patients with disease flare from those with infection. An optimized multivariable logistic regression model revealed that an elevated ESR:CRP ratio (>1.17), low white blood cell (WBC) count (<6.25 × 10<sup>9</sup>/L), low absolute neutrophil count (<5.55 × 10<sup>9</sup>/L), and low CRP (<113 mg/L), C3 (<44.5 mg/dL), and C4 (<13.5 mg/dL) levels helped discriminate disease flare from culture-positive infection. These laboratory parameters yielded areas under the receiving operating characteristic curve of 0.87 (95% confidence interval [CI] 0.76-0.97) for flare versus culture-positive infection and 0.94 (95% CI 0.88-1.00) for flare versus culture-negative infection. These optimized models, using multiple laboratory parameters, significantly outperformed the ESR:CRP ratio alone (P < 0.02) in discriminating flare from infection.</p><p><strong>Conclusion: </strong>The ESR:CRP ratio plus C3 and C4 levels, WBC count, neutrophil count, and monocyte count discriminate flare from either culture-positive or culture-negative infection in febrile patients with SLE. Our findings warrant prospective validation.</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 6","pages":"e70051"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12159916/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70051","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The objective of this study was to assess clinical laboratory parameters that distinguish between disease flare and infection in febrile patients with systemic lupus erythematosus (SLE) at safety-net hospitals in Los Angeles.
Methods: We reviewed electronic medical records of patients admitted from August 1, 2016, through July 31, 2019, categorizing them as disease flare, bacterial infection (culture positive), culture-negative infection, and both flare and infection. Laboratory parameters collected within 48 hours of admission (complete blood cell count with differential, liver function panel, erythrocyte sedimentation rate [ESR], C-reactive protein [CRP], C3, C4, lactate, procalcitonin, and ferritin) were analyzed.
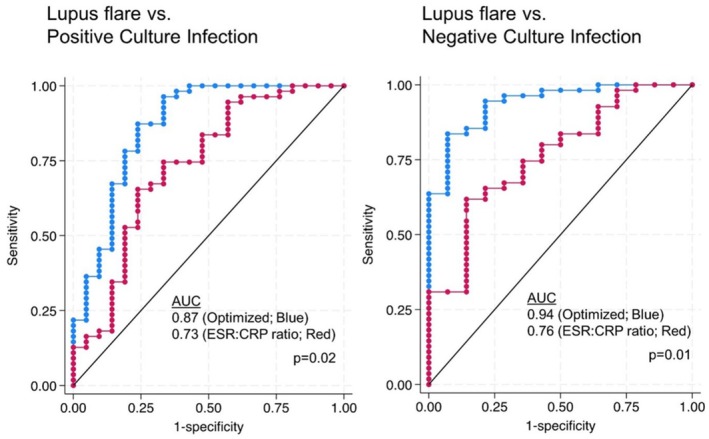
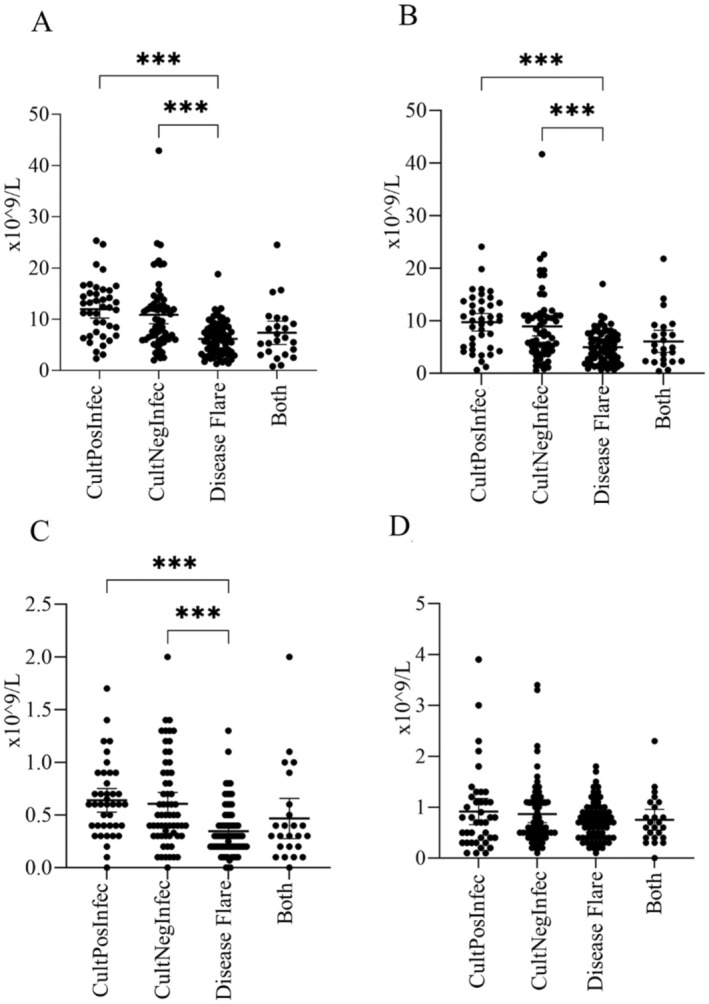
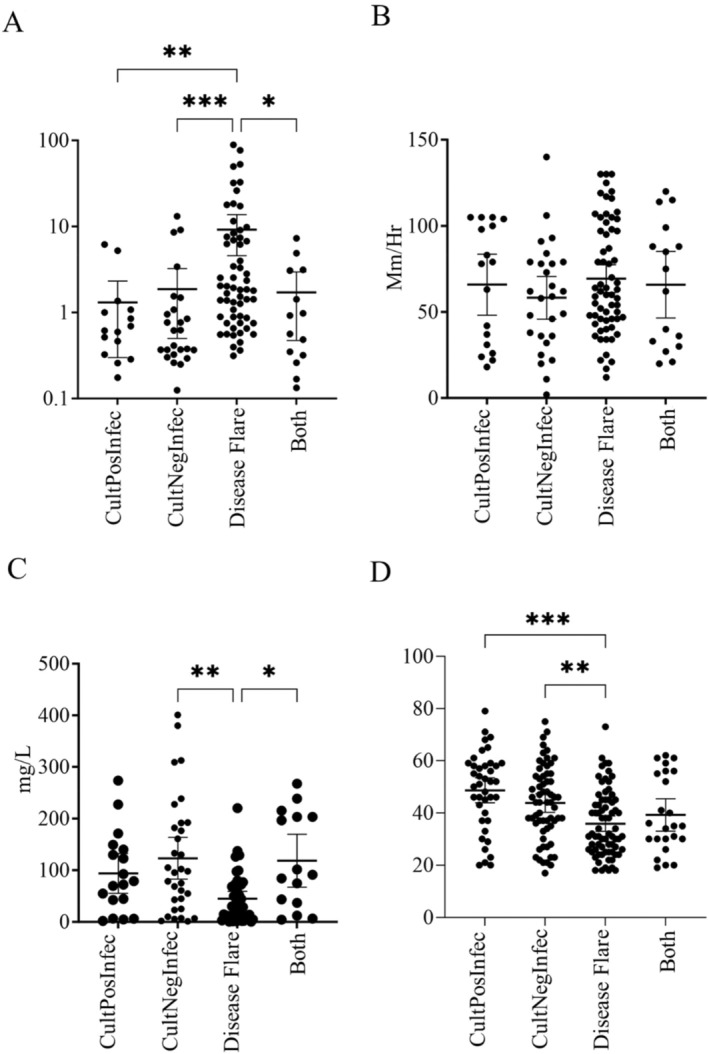
Results: Several laboratory parameters significantly distinguished febrile patients with disease flare from those with infection. An optimized multivariable logistic regression model revealed that an elevated ESR:CRP ratio (>1.17), low white blood cell (WBC) count (<6.25 × 109/L), low absolute neutrophil count (<5.55 × 109/L), and low CRP (<113 mg/L), C3 (<44.5 mg/dL), and C4 (<13.5 mg/dL) levels helped discriminate disease flare from culture-positive infection. These laboratory parameters yielded areas under the receiving operating characteristic curve of 0.87 (95% confidence interval [CI] 0.76-0.97) for flare versus culture-positive infection and 0.94 (95% CI 0.88-1.00) for flare versus culture-negative infection. These optimized models, using multiple laboratory parameters, significantly outperformed the ESR:CRP ratio alone (P < 0.02) in discriminating flare from infection.
Conclusion: The ESR:CRP ratio plus C3 and C4 levels, WBC count, neutrophil count, and monocyte count discriminate flare from either culture-positive or culture-negative infection in febrile patients with SLE. Our findings warrant prospective validation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


